Case Report
Hemangioma of Uterus - A Rare Case Report
Nagure PV1, Jadhav PL2, Nikam VR3*, Mane AD4 and Patil JK2
1Department of Radiodiagnosis, Prakash Institute of Medical Sciences, Consultant Radiologist at Eureka Diagnostic Centre, India
2Department of Radiodiagnosis, D.Y. Patil Medical College, India
3Department of Anatomy, D.Y. Patil Medical College, India
4Consulting Oncopathologist, Aster Aadhar Hospital, India
Corresponding author: Nikam VR, Department of Anatomy, D.Y. Patil Medical college, Dr. DY Patil Education Society, Deemed to be University Kasaba Bawada, Kolhapur, India, Tel no: +91-9665730990; E-mail: dr.vasudhanikam@gmail.com
Citation: Nagure PV, Jadhav PL, Nikam VR, Mane AD, Patil JK. Hemangioma of Uterus - A Rare Case Report. Indian J Appl Radiol. 2019;5(1): 132.
Copyright ©2019 Nagure PV, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Applied Radiology | Volume: 5, Issue: 1
Submission: 26/12/2018; Accepted: 31/01/2019; Published: 04/02/2019
Abstract
Cavernous hemangiomas of the uterus are extremely rare, benign lesions associated with gynaecological complications. They may be either localised presenting as an endometrial polyp or a uterine mass in which most of the uterine wall is composed of enlarged vascular spaces replacing the normal myometrium. Here we report the imaging findings of such rare case of hemangioma in 25 years old non-pregnant female.
Keywords: Endometriosis; Menorrhagia; Uterus; Antenatal Diagnosis; Polyp
Introduction
Hemangioma is a benign tumour originating from the endothelial cells of the blood vessels or from the pericytes located on the outer side of the vascular wall [1]. They appear in the two forms as capillary hemangioma and cavernous hemangioma. Capillary hemangiomas are usually found on the skin. They can have different size and shape, from very small to very large ones, whose occurrence may cause aesthetic disturbance. Cavernous hemangiomas can be found on the skin as well as in the parenchymatous organs such as liver, kidney, breast muscle, intestine wall, brain and bones. Both types of hemangiomas can be found in uterus but very rarely [2].
Cavernous hemangiomas of the uterus are extremely rare benign lesions. About 5 cases of this disease were found in the literature over the last century. Although they can be found at all levels of the uterine wall, including the serosa, myometrium and endometrium, most cases usually involve the myometrium diffusely [3,4]. Because of their small size and their asymptomatic nature, majority of hemangiomas are discovered incidentally, but they may have abnormal vaginal bleeding [4].
A cavernous hemangioma of the uterus is mostly described in pregnant women presenting with uncontrolled bleeding or pain [5,6].
Some extreme localization such as clinical region or adenomyotic foci in the uterus has been reported for uterine hemangiomas [7].
Here we report the imaging findings of this rare lesion in 25 years old non-pregnant female.
Case Report
A 25 years old female was referred for imaging to the hospital. There was history of polymenorrhagia and pelvic pain since last two years. The patient had the complaints of constant, dull aching pain in lower abdomen which increases at night. Two years back her menstrual cycles were of 28 days with normal bleeding of 3-4 days. Since last two years she is complaining of intermenstrual bleeding which is significantly increased since few months. The patient complained of feeling of fullness in the vaginal canal.
On physical examination the patient was pale. Per abdomen examination was unremarkable.
Per vaginal examination revealed red to pinkish mass in the upper vaginal canal with prominent surface vessels which were bleeding on touch. The patient was advised for pelvic ultrasound and MRI.
Ultrasonography of the pelvis revealed a solid mass with prominent vascularity in cervical/ upper vaginal canal. It has multiple hypoechoic spaces within.
To know the exact origin of the mass as well as its extension, Magnetic Resonance Imaging of pelvis was done which revealed a polypoidal mass within the fornix and upper vaginal canal. The mass shows predominately hyperintense signal on T2 weighted images and hypointense signal on T1 weighted images. There were multiple haemorrhagic spaces within the lesion appearing hyperintense on T1 weighted images and mixed signal intensity on T2 weighted images. Few of these spaces showing fluid-fluid levels. There was a central fibro vascular stalk attached to the posterior endometrial wall (Figure 1a and Figure 2a).
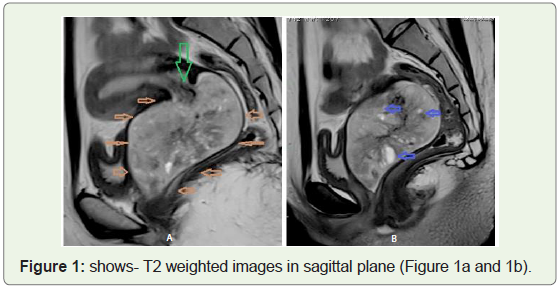
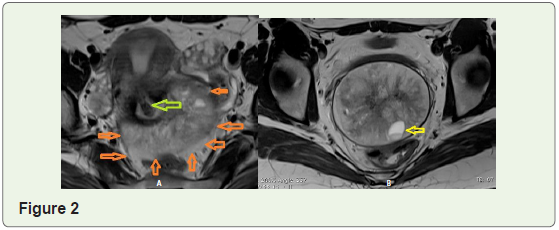
Figure 1 shows- T2 weighted images in sagittal plane shows a large polypoidal mass filling the fornix and vaginal canal (lined by orange arrows) (Figure 1a and 1b). It displays bright signal on T2 weighted image. Also note multiple vascular spaces in the lesion denoted by blue arrows in Figure 1b.
The lesion was attached to the posterior endometrial lining of the uterus by fibro vascular stalk denoted by green arrow in Figure 1a.
T2 weighted axial images shows the mass within the fornix, vaginal canal (denoted by orange arrows) (Figure 2a). Also note the fibro vascular stalk attached to posterior endometrial wall (denoted by green arrow) and haemorrhagic spaces (denoted by yellow arrow) (Figure 2b).
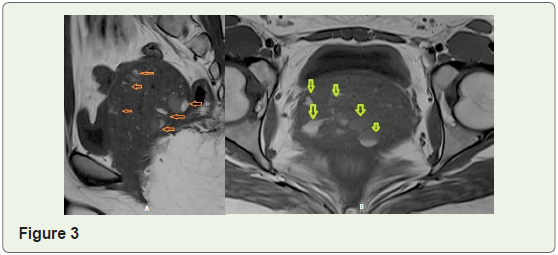
Figure 3 shows T1 sagittal (Figure 3a) and T1 axial (Figure 3b) image showing the lesion being predominately hypointense with vascular spaces/ intra-lesioned haemorrhages denoted by orange and yellow arrows. Also note the fluid-fluid levels within the vascular spaces.
Considering the macroscopic appearance and history of bleeding per vaginally possibility of vascular polyp and polypoidal lesion with vascular spaces like cavernous hemangioma were considered in the differential diagnosis.
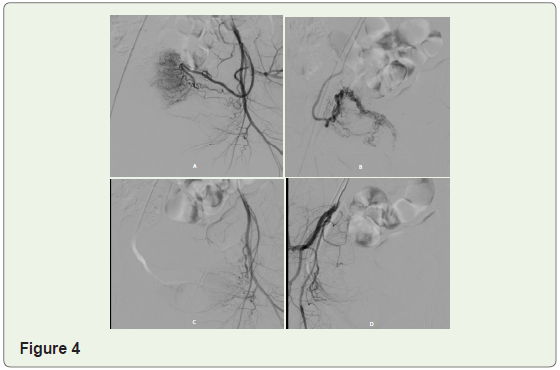
For further management the patient was referred to gynaecologist. To decrease the intraoperative loss preoperative angio-embolization was done.
Selective angiogram shows enlarged right and left uterine arteries supplying the lesion (Figure 4a and Figure 4b respectively) with prominent arterial blush. Figure 4c and Figure 4d represent post embolization status with absence of blush.
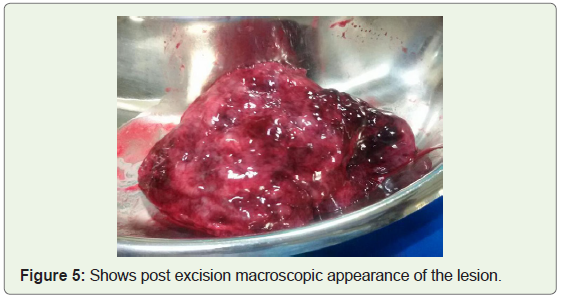
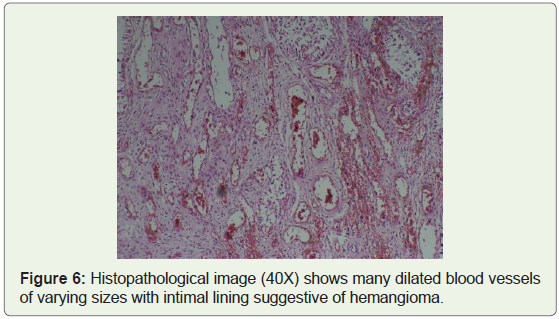
After pre-operative embolization, hysteroscopic excision of polypoidal lesion was done (Figure 5). The histopathological examination proved the lesion to be hemangioma (Figure 6).
Discussion
Clinically hemangioma of uterus is impressive myoma, they are asymptomatic. However extensive bleeding can occur. Ultrasonography finding points out the enlarged uterus with occurrence of cavernous change of echotexture. MRI and CT are used as additional to USG diagnosis [2]. In our case USG was not conclusive hence, we used MRI as an additional tool for the diagnosis.
Based on the review of literature it can be suggested that a cavernous hemangioma has no predilection for age and that its relationship to pregnancy is coincidental [3].
Both types of hemangiomas capillary and cavernous are found in the uterus. Capillary hemangiomas are limited to endometrium and cervix while the cavernous forms affect all coats of the uterus [4]. In our case there was cavernous hemangioma. The most atypical feature of our case is that the lesion presented as polypoidal mass with stalk mimicking an endometrial polyp. Adding to the further confusion was it was presented as upper vaginal mass which further found to be arising from the endometrium.
Presentation of uterine hemangioma in non-pregnant women may be due to gradual increase in size of pre-existing lesion following pregnancy [6]. In our case also this reason can be considered.
All the cases of endometrial hemangiomas described in the literature to date have shown progressive symptoms of uterine bleeding which do not respond to conservative therapy [8]. In our case also patient did not respond to conservative treatment and hence was referred for MRI imaging.
The definitive diagnosis relies on the final histologic examination. Nonetheless the uterus may appear pulsatile on examination, ultrasonography, pelvic angiography or computed tomography could confirm the vascular nature of the lesion if there is clinical suspicion for this abnormality, MRI could serve as an additional imaging modality for diagnosis [9,10]. Our patient also initially had undergone ultrasonography, later the diagnosis was confirmed by imaging with MRI.
Conclusion
We present a rare case of cavernous hemangioma of the uterus presenting as a polypoidal mass with stalk. As it is rare vascular tumour and this condition should be kept in mind in differential diagnosis of the patients with abnormal vaginal bleeding with lesion showing prominent vascularity and haemorrhagic spaces within.
Acknowledgement
This work was supported by Eureka Diagnostic Centre; Kolhapur, Aster Aadhar Hospital, Kolhapur and D.Y. Patil Education Society; Deemed to be University; D.Y. Patil Medical College; Kolhapur.
Thanks to Chancellor, Vice Chancellor, Pro Vice Chancellor, Registrar and Dean of D.Y. Patil Education Society’s deemed to be University and D.Y. Patil Medical College, Kolhapur. Thanks to Dr. Pramod Nagure, Dr. Prithviraj Jadhav, Dr. Ashwini Mane, Dr. Jeetendra Patil and my colleagues of Department of Anatomy for their support.
References
- Esmer AC, Ozsurmeli M, Yuksel A, Kalelioglu I, Has R, et al. (2014) Antenatal sonographic diagnosis of diffuse cavernous hemangioma of the uterus. Marmara Med J 27: 134-137.
- Mastilovic K, Rajovic J, Zikic D, Stojiljkovic B (2005) Hemangioma of the uterus. Arch Oncol 13: 148-149.
- Agarwal M, Agarwal A, Bhadani P, Kumar K (2016) Localized cavernous hemangioma of uterus: A rare cause of abnormal uterine bleeding. J Case Rep 6: 388-390.
- Aka KE, Apollinaire Horo G, Fomba M, Kouyate S, Koffi AK, et al. (2017) A rare case of important and recurrent abnormal bleeding in a post partum woman caused by cavernous hemangioma: A case report and review of literature. Pan Afr Med J 28: 130.
- Saeed-Vafa D, Myers E, Huang Y, Ferriss JS, Manucha V (2011) Localized cavernous hemangioma of the uterus involving adenomyotic foci. J Cancer Res Ther 7: 69-71.
- Celik ZE, Bastoklu S, Ilhan TT, Celik C (2017) Cavernous hemangioma arising in an intramural leiomyoma. Integr Cancer Sci Therap 4: 1-3.
- Riggs J, Bertoni M, Schiavello H, Weinstein A, Kazimir M (2003) Cavernous hemangioma of the cervix with intractable bleeding: A case report. J Reprod Med 48: 741-743.
- Benjamin MA, Yaakub HR, Telesinghe P, Kafeel G (2010) A rare case of abnormal uterine bleeding caused by cavernous hemangioma: a case report. J Med Case Rep 4: 136.
- Chou WY, Chang HW (2012) Uterine hemangioma: a rare pathologic entity. Arch Pathol Lab Med 136: 567-571.
- Virk RK, Zhong J, Lu D (2008) Diffuse cavernous hemangioma of the uterus in a pregnant woman: report of a rare case and review of literature. Arch Gynecol Obstet 279: 603-605.