Case Report
Clinico Radiological Constellation of a Novel Neurocutaneous Syndrome- Tuberous Sclerosis- A Rare Case Report
Nikam V1*, Shettennavar M2 and Babanagar S3
1Department of Anatomy, D.Y. Patil Medical College, India
2S.M Diagnostic and Research Centre, India
3Department of Radiodiagnosis, D.Y. Patil Medical College, India
Corresponding author: Nikam V, Department of Anatomy, D.Y. Patil Medical college, Dr. DY Patil Education Society; Deemed to be University Kasaba Bawada; Kolhapur, India, Tel no: 9665730990; E-mail: dr.vasudhanikam@gmail.com
Citation: Nikam V, Shettennavar M, Babanagar S. Clinico Radiological Constellation of a Novel Neurocutaneous Syndrome- Tuberous Sclerosis- A Rare Case Report. Indian J Appl Radiol. 2018;4(1): 128.
Copyright ©2018 Nikam V, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Applied Radiology | Volume: 4, Issue: 1
Submission: 30/08/2018; Accepted: 05/11/2018; Published: 09/11/2018
Abstract
Tuberous sclerosis complex is a genetic multisystem disorder. It is an autosomal disorder affecting multiple organs. It is characterised by the growth of multiple hamartomas in several organs such as brain, kidney, skin, uterus and liver. It is caused by mutation of either TSC1 or TSC2 gene encoding hamartin and tuberin respectively. We report a case of 50 years old female with tuberous sclerosis complex who presented with facial angiofibromas, angiomyolipomas of bilateral kidney, subependymal nodules and subependymal giant cell astrocytoma. The aim of the study is to present clinical and radiological features in a patient who exhibited multiple hamartomas of various organ systems.
Keywords: Cortical tubers; Facial angiofibromas; Genetic disorder; Renal angiomyolipomas; Subependymal nodules; Tuberous sclerosis
Introduction
Tuberous Sclerosis complex is a genetic disorder of hamartoma formation in many organs particularly the skin, brain, eye, kidney, heart and other organs, leading to significant health problems like seizures, intellectual disability, autism or developmental delay [1,2]. Tuberous sclerosis complex also known as Bourneville disease; is an autosomal dominant neurocutaneous, multisystem disorder [3,4]. Von Recklinghausen first described tuberous sclerosis in 1862. Desire Magloire Bourneville a French physician formulated the term sclerose tubereuse, from which the name of the disease has evolved. Sherlock coined the term ‘EPILOIA’ encompassing the clinical trial of tuberous sclerosis (Epi: epilepsy, Loi: low intelligence, A: adenoma). As the manifestations of the disease are variegated in nature, the term Tuberous Sclerosis Complex (TSC) is widely used [5].
It is an autosomal dominant inherited disease being associated with at least two separate chromosomes TSC1 found on chromosome 9q34 and TSC2 on chromosome 16p3. There is family history of disease in 50% of affected patients with an autosomal mode of inheritance. Some individuals acquire tuberous sclerosis complex through a process called gonadal mosaicism. TSC is caused by defects or mutation in two genes TSC2 and TSC2. Only one of the genes needs to be influenced to produce the disease. The TSC1 gene is located on chromosome 9q34 and produces a protein hamartin. The TSC2 gene is on chromosome 16p3 and produces tuberin [5].
It was German paediatric neurologist; Heinrich Vogt in 1908 consolidated three different aspects of facial rash, the intellectual deficits, and the seizures; of tuberous sclerosis into a unifying diagnostic classification known as Vogt’s triad of epilepsy, mental insufficiency and adenoma sebaceum [6]. Vogt’s diagnostic triad defined the condition for next 60 years, until it was superseded by the monograph published by Manuel Gomez in 1979, which described for the first time the full clinical spectrum of tuberous sclerosis complex [7].
Though it was first identified as an autosomal dominant disorder 60-70% cases can be due to spontaneous mutations. The incidence of tuberous sclerosis is undetermined. The point of prevalence TSC ranges from 1:6000 to 1:10000 individuals and the diagnosis is usually established between 4-10 years of age or in puberty [8]. The radiological hallmarks of this neurocutaneous syndrome are universally accepted as enough for diagnosis [9].
Here we report a case of 50 years old female with TSC presented with mental retardation, seizures, adenoma sebaceum over face, ungual fibromas over fingers and toes, subependymal giant cell astrocytoma, cortical tubers, and subependymal nodules.
Case Report
A 50-year-old female was referred for screening, presented with chief complaints of multiple nodules over the face, nose and in the nail beds of both hand and feet. There was history of recent onset of headache and vomiting. The patient had history of chronic epilepsy. The patient had history of chronic epilepsy.
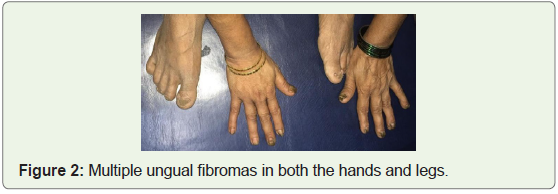
On physical examination the patient was pale with facial angiofibromas (Figure 1), and ungual fibromas involving hands and feet (Figure 2).

There was no family history of such disease in previous generations. Ultrasonography of abdomen and MRI brain was advised.
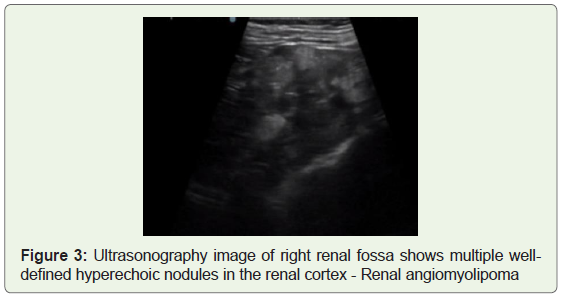
Ultrasonography abdomen revealed bulky kidneys with hyperechoic nodules of varying sizes scattered throughout the renal parenchyma suggestive of angiomyolipomas (Figure 3). There were multiple cysts of varying size filled with fluid measuring about 5-20 ml in both the kidneys.
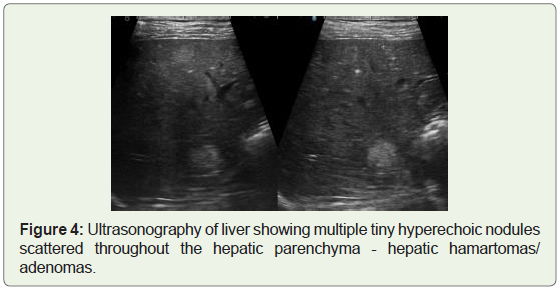
There were multiple tiny hyperechoic nodules throughout the liver parenchyma which were suggestive of hamartomas/ angiomyolipomas (Figure 4).
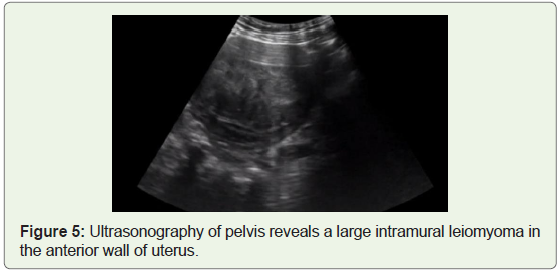
Screening of pelvic cavity revealed a well-defined heterogenous area in the uterus measuring about (8 cms in length x7 cms in breadth), involving the fundus and body of uterus suggestive of leiomyomas (Figure 5).
All these imaging findings were suggestive of spectrum of pathologies involving abdominal organs in tuberous sclerosis.
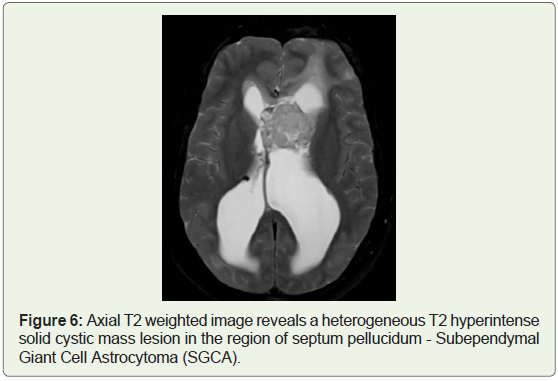
MRI brain study revealed well defined heterogeneous T2 hyperintense mass lesion along the left lateral aspect of septum pellucidum in the frontal horn and the left lateral ventricle extending to foramen of Monro measuring about (3.5 cms in length x3 cms breadth x3.2cms in height), it appeared intermediate signal intensity on T1 weighted images and shows evidence of restricted diffusion on diffusion weighted images (Figure 6).
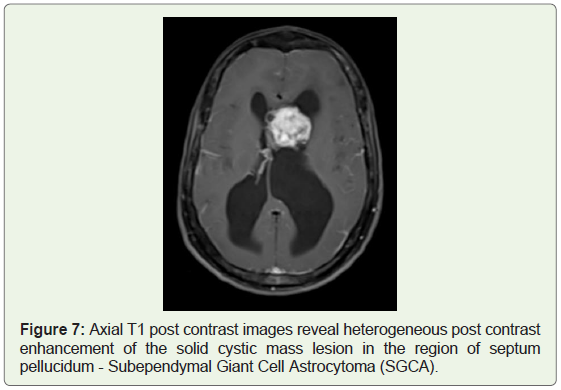
Few tiny specks of blooming were seen within the lesion. Post contrast study revealed heterogeneous post contrast enhancement of the solid cystic mass lesion in the region of septum pellucidum - suggestive of intraventricular neoplastic lesions, subependymal giant cell astrocytomas (Figure 7).
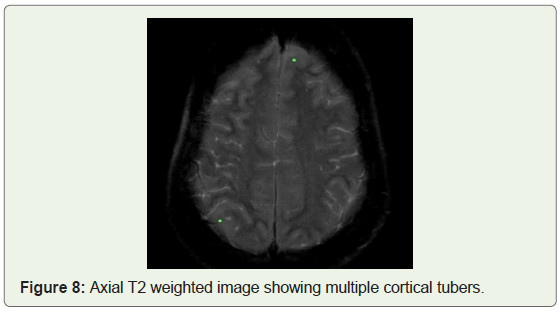
Few tiny hypointense subependymal nodules were seen in the lateral subependymal region of both the lateral ventricles. Multiple patchy areas of T2/FLAIR hyperintense lesions were seen in bilateral frontoparietal, occipital and temporal cortices and right posterior inferior cerebellar cortex representing cortical tubers (Figure 8).
There was moderate hydrocephalus with dilatation of lateral ventricles with significant dilatation of left lateral ventricle. CSF seepage was seen along the frontal horns of both lateral ventricles. 3rd and 4th ventricles appeared normal.
Few findings were noticed in the remaining part of cerebral cortex such as effacement of cerebral cortical sulci and basal cisterns, multiple cortical tubers in the cerebral cortex.
These all imaging findings represent changes of neurocutaneous syndrome known as tuberous sclerosis.
Discussion
Tuberous sclerosis is an autosomal disorder which affects the patient as well as family members in various ways. It is a disorder of cellular differentiation and proliferation that can affect the brain, skin, kidney and other organs. Many of the clinical features result from hamartomas, particularly in kidney and brain [1]. In our patient also, multiple tiny hamartomas were present in multiple organs such as kidney, uterus, brain, face and fingers.
TSC is caused by mutation on either of two genes TSC1 and TSC2 which encode the proteins hamartin and tuberin respectively. These proteins act as tumor growth suppressor agents that regulate cell proliferation and differentiation. In majority of cases there was probable diagnosis with one major plus and one minor positive feature [2,3]. However, in our case 8 major and 4 minor criteria were present, which strongly suggest TSC. In our patient TSC was most likely due to spontaneous mutation which is very commonly seen in a greater number of patients as there was no history of such disease in previous generations.
The patient suffering from TSC as per diagnostic criteria of 2012 international tuberous sclerosis complex consensus conference, have following symptoms such as hypertension and are non-diabetic. They fulfill 5 major criteria including facial angiofibromas, periungual fibromas, cortical dysplasia, subependymal nodules and renal angiomyolipoma [4]. In our patient these all major criteria were seen which strongly supports the diagnosis of TSC.
Further the triad of symptoms of tuberous sclerosis are described by Vogt, which consists of seizures, adenoma sebaceum (facial angiofibromas) and mental retardation. Not all patients have this classic traid however and half of the patients are of normal intellect and quarter do not have seizures [5]. In our case the classical triad was present, and the patient had history of chronic seizures.
Usually two types of renal lesions are seen in the patients with tuberous sclerosis, angiomyolipomas and renal cyst. They may be unilateral, bilateral, single or multiple [8]. In our case angiomyolipomas were present in bilateral kidneys.
CNS involvement includes cortical tubers, subependymal nodules, subependymal giant cell astrocytoma and benign white matter lesions. Subependymal nodules are found in 95% of patients with tuberous sclerosis. Subependymal giant cell astrocytomas are histologically benign tumors located near the foramen of Monro. Associated obstructive hydrocephalus is a common sign in patients with tuberous sclerosis [9]. In our patient also all these symptoms were positively seen along with subependymal giant cell astrocytoma near the foramen of Monro. Our patient had moderate hydrocephalus with dilatation of lateral ventricles.
The respiratory system is rarely impaired with less than 1% of patients presenting with direct lung involvement due to tuberous sclerosis [10]. In our patient the medical history, investigations did not reveal any evidence for systemic involvement of lungs and heart.
The prognosis of the disease depends upon the severity or the multiple organ involvement such as; brain, kidney, skin; so long-term management is required. There is no cure for tuberous sclerosis complex. Hence for further management the patient was referred to neurosurgeon.
Conclusion
Tuberous sclerosis complex is a lifelong condition therefore individuals should be monitored at regular intervals by experienced clinicians only. The dermatologic manifestations of tuberous sclerosis are helpful in the diagnosis of this disorder. Early diagnosis is very important for proper management of the disease. However, radiology plays a key role in diagnosis and detecting the complex nature of the disease.
The quality of life for the patient can be improved by thorough clinical and radiological evaluation, continuous monitoring of the symptoms, family planning and genetic counselling.
Declarations
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Conflict of interest
The authors have disclosed no potential conflicts of interest, financial or otherwise.
References
- Chandrakala, Patil S, Guruprasad KY (2014) A case report of tuberous sclerosis in two generations. J Assoc Physicians India 62: 60-64.
- Syed KN (2010) Tuberous sclerosis - Case report. J Pak Med Assoc 60: 683-685.
- Chenguang L, Songjie L, Jian Y (2015) Tuberous sclerosis complex confirmed by genetic analysis: A Case Report. J Neurol Neurosci 6: 1-3.
- Butt DS, Kamran M, Ussaid A, Ullah Z, Butt KI (2017) Tuberous sclerosis complex- Case report and management by multidisciplinary approach. J Pakistan Association of Dermatol 27: 301-305.
- Kunwarpal S, Amritpal S, Sukhdeep K, Kulvinder S, Thukral CL (2013) Tuberous sclerosis: A case report with review of literature. J Evol Med Dent Sci 2: 8752-8759.
- Curatolo P (eds) (2003) Tuberous sclerosis complex: from basic science to clinical phenotypes. London: Mac Keith Press.
- Goodricke S (2015) Focal point: The road to Vogt’s Triad. Lancet Neurol 14: 690.
- Debbarma RK, Chakma K (2015) Tuberous sclerosis in young female-A rare case report. IOSR J Dent Med Sci 14: 58-61.
- Patel SB, Shah SS, Goswami K, Shah N, Pandhi S (2004) Case report: Tuberous sclerosis - it’s varied presentations. Ind J Radiol Imag 14: 423-425.
- Bryson E, Neustein S (2006) Tuberous sclerosis: A case report and review. The Internet J anesthesiology 13: 1-4.