Research Article
Study of Abdominal Manifestations by USG in HIV/AIDS Patients
Sharma M1*, Bahadur L2, Sharma S3, Sagar D1 and Modi V1
1S N Medical College, India
2MRCP Edinburg, UK
3V A Hospital West Palm Florida, USA
Corresponding author: Sharma M, S N Medical College, Agra, India, E-mail: drmadhusharmaagra01@gmail.com
Citation:Sharma M, Bahadur L, Sharma S, Sagar D, Modi V. Study of Abdominal Manifestations by USG in HIV /AIDS Patients. Indian J Appl Radiol. 2018;4(1): 126.
Copyright ©2018 Sharma M, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Applied Radiology | Volume: 4, Issue: 1
Submission: 01/08/2018; Accepted: 17/09/2018; Published: 20/09/2018
Abstract
The major target of HIV is the immune system and the abdominal pathologies are second most commonly found in patients of AIDS after pulmonary manifestations. These abdominal manifestations are on increase may be due to immunocompromised status of these patients and due to antiretroviral therapy which has increased life expectancy in these patients.
Purpose of this study is to describe abdominal findings and to evaluate clinical utility of USG in HIV patients with the use of abdominal probe, high frequency probe and Color Doppler USG.
Ultrasonography is easy to perform It is noninvasive and safe imaging modality easily available in high prevalent zones of AIDS where CT And MRI are not available and are not affordable for patients making them 2nd and 3rd choice of investigating modality.
This study includes 60 HIV patients, 37 patients were male and 23 patients were female. Age group studied was 20 yrs to 65 yrs in Department of Radiodiagnosis SNMC Agra referred from ART Department of this hospital from 30.1.2014 to 3.6.2014, almost 4 months duration. Most prevalent age group was from 40 - 49 yrs that was 23 patients, next was 30 - 39 yrs i.e. 20 patients, third in declining order was 20 - 29 yrs i.e. 12 patients and less prevalent age groups were from 50 - 59 yrs and above 60 - 70 yrs.
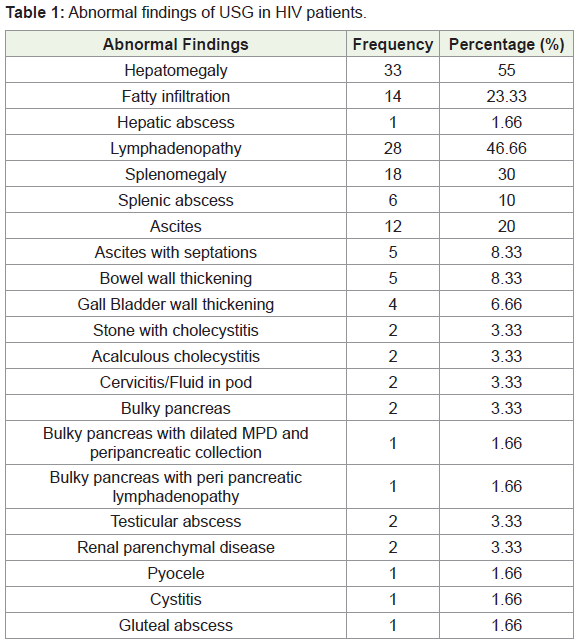
These patients had diverse abdominal findings. Out of 60 patients 3 had no abdominal findings. Hepatomegaly was found in 33 patients, fatty hepatic changes in 14 patients and in one case there was Hepatic abscess.
Lymphadenopathy was found in 28 cases. Splenomegaly was found in 20 cases and in 6 cases there were also having splenic abscesses. Ascites was found in 12 cases it was septated and non septated ascites. Cholecystitis in 4 cases. Bowel wall thickening in 5 cases in most of cases it was thickening of ileum and Ileocaecal junction thickening. Other findings were renal parenchymal disease in 2 cases, Bulky pancreas in 2 cases, cervicitis in 2 cases, one case each of cystitis and pyocele. Testicular abscess in 2 cases and gluteal abscess in one case along with other abdominal findings. Many patients had two or more pathologies.
Keywords: Immunocompromised; Prevalence; Lymphadenopathy; Hepatomegaly; Splenic abscesses; Bowel wall thickening
Introduction
The Acquired Immune Deficiency Syndrome is a clinical entity resulting from HIV infection and remains matter of a major public health and social concern. The target of HIV infection is immune system. The frequency of abdominal disorders in HIV/AIDS patients has been reported to be second only to pulmonary disease. This cytopathic retrovirus destroys immune system and leads to opportunistic infections and tumors. Sex workers are at highest risk of AIDS.
National AIDS Control Organisation (NACO) launched National AIDS control programe in 1992. There after NACP I, II, III, IV were launched IN 1999, 2007, 2012-2017.
Programe in 1992 was focused on the national HIV surveillance system, prevention activities among High Risk Groups (HRGs) including information on HIV and the blood safety programs.
India had 3rd largest epidemic of AIDS in 2016 due to its large population. Three states with highest prevalence, Manipur, Mizoram, and Nagaland. Some of Northern states are also having high prevalence.
NACO 2015 Avert.org - As per the recently released, India 2015 report, HIV Estimation National adult 15-49 yrs HIV prevalence in India is estimated at 0.26% (0.22% - 0.32%), 0.30% among males and at 0.22% among Females. The adult HIV prevalence has steady decline from an estimated peak of 0.38% in 2001 - 2003 through 0.34% in 2007 and 0.28% in 2012 to 0.26% in 2015.
Ultrasound is easily available and affordable to patient’s plays significant role in diagnosis follow up and doing interventional procedures in patients of HIV positive patients. Also USG helps in assisting approach toward therapy. The early detection of comorbidities for which USG is useful includes Tumors, Infections. Inflammatory, Metabolic and Degenerative changes.
Other modalities like CT and MRI help in better defining and characterizing HIV related abdominal findings but they are less available at periphery in area of high prevalence and cost effective, makes them 2nd or 3rd choice of radiological investigations, Also for follow up USG is most preferred modality.
CD4 count is a good index for monitoring progression of disease as degree of immunosuppression is related to level of CD4 Count and various manifestations which occur as a result of opportunistic infections, such as tubercular, fungal, CMV. Various tumors, which are associated with HIV e.g. NHL, Burkitt’s lymphoma, Kaposi sarcoma, Cervical cancer.
Aims and Objectives
To study abdominal ultrasound findings in HIV positive patients.
Material and Method
This study is an observational study carried out in Department of Radiodiagnosis SNMC AGRA.
It is a short term study of almost 4 months duration 30.1.2014 - 3.6.202014. Total no of 60 cases studied, referred from ART center of our college - hospital.
This study was carried out on machine Medison both convex and linear probes were used of frequency 4.5 MHz and 7.5 MHz respectively. Patients were asked to come after overnight fasting of 12 hrs so as to reduce bowel artifacts. Examination was performed with due consent in supine and lateral positions.
USG and X-rays were done in our facility for early detection of abnormality.
Inclusion criteria were seropositive patients and age of patient above 20 yrs.
Exclusion criteria was patients who did not give consent for keeping record due to social reasons, patients with incomplete examination and age under 20 yrs.
HIV/AIDS is known to have wide variety of clinical manifestations with involvement of various systems/organs. USG is a versatile tool used for abdominal imaging affected by disease.
Immunosuppression with USG we can evaluate all abdominal organs and with the use of high frequency probe retroperitoneum can also be evaluated properly. Color Doppler adds further information like vascularity of organs, nodes and the lesions. Guided biopsies give cytohistological information of pathologies.
We recorded data on paper in a register which later on transferred to computer where it was stored throughout period of study. Criteria for lymphadenopathy - Enlarge Lymph Nodes > 1 cms in short axis diameter.
Splenomegaly -Splenic span > 12 cms
Hepatomegaly ->13.5 -15 cms in mid clavicular line in adults, craniocaudal length [1,2]. CBD diameter 5 - 7 mm depending on age of patient in most distils aspect of head of Pancreas. Electronic calipers were used AP diameter from inner border to inner border. Color Doppler was used to confirm vascular and ductal anatomy.
AIDS is multisystem disease buts its demographic, clinical and sonographic pattern remains same globally. Other imaging modalities especially CT can explore abdominal organs in more detail than USG. But as it is expensive, less readily available in high disease prevalent areas and due to its radiation hazard makes it second choice of investigation. Also results obtained with CT are comparable to results obtained with USG.
Observations
This study includes 60 HIV patients, 37 patients were male and 23 patients were female. Age group studied was 15 yrs to 65 yrs in Department of Radiodiagnosis SNMC Agra referred from ART Department of this hospital from 30.1.2014 to 3.6.2014, almost 4 months duration. Most prevalent age group was from 40 - 49 yrs that was 23 patients, next was 30 - 39 yrs i.e. 20 patients, third in declining order was 20 - 29 yrs i.e. 12 patients and less prevalent age groups were from 50 - 59 yrs and above 60 - 70 yrs. These patients had diverse abdominal findings out of 60 patients 3 had no abdominal findings. Most of patients had two or more findings.
Hepatomegaly was found in 33 patients, fatty hepatic changes in 14 patients and in one case there was associated Hepatic abscess. Lymphadenopathy was found in 28 cases they were intraperitoneal, retroperitoneal and iliac group of nodes. Splenomegaly was found in 20 cases and in 6 cases there were splenic abscesses. In 5 cases abscesses were small and one there was large abscess as 18 mm. Ascites was found in 12 cases it was septated and non septated ascites. Cholecystitis in 4 cases, calculous and Acalculous Cholecystitis. Bowel wall thickening in 5 cases in most of cases it was thickening of ileum and Ileocaecal junction. Other findings were Renal parenchymal disease found in 2 cases. Bulky pancreas was seen in 2 cases in one there was dilated MPD as 5mm along with peripancreatic nodes. Cervicitis found in 2 cases, one case each of cystitis and pyocele. Testicular abscess in 2 cases and gluteal abscess in one was found along with other abdominal findings ((Table 1)).
Discussion
Abdominal symptoms are most common complaint of HIV patients. Precise diagnosis based on symptoms alone is very difficult. Hence radiological investigations especially USG plays significant role in reaching diagnosis [3].
Hepatomegaly was most common finding in our study, As 33 patients out of 60 were having Hepatomegaly with or without fatty infiltration and were having other sonological findings also. 14 pts were having fatty infiltration and one was having hepatic abscess.
Fatty infiltration was observed as increased parenchymal echogenicity (Figure 1a and 1b).
Also there was large association of deranged liver functions and altered echotexture in patients of hepatitis B and C [4]. Among the tumors, there are cases reported of Lymphoma and HCC involving Liver In patients of AIDS. Due to HAART therapy which has prolonged life span of HIV patients there is hepatomegaly with deranged liver function test. Liver echotexture may be coarse with granulomas.
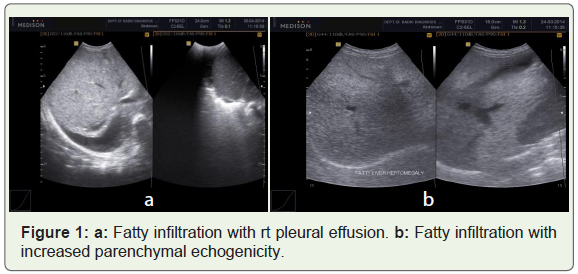
Lymphadenopathy was second most common finding due to compromised immune status [5]. We have found 28 patients with enlarge lymph nodes. The criteria of enlarge node was short axis diameter 10mm or more. Enlarge nodes were round or oval. They were found at Peripancreatic region (Figure 2a), Porta (Figure 2b), Paraaortic region, Mesenteric or in right iliac fossa (Figure 2c). Sonologically enlarge nodes with central echogenic hilum with increased vascularity was seen in cases of adenitis.
In patients of tuberculosis nodes were hypoechoic or anechoic having central Caseation. Nodes were scanned with convex and high frequency probes both. Color Doppler was used to see vascularity of nodes.
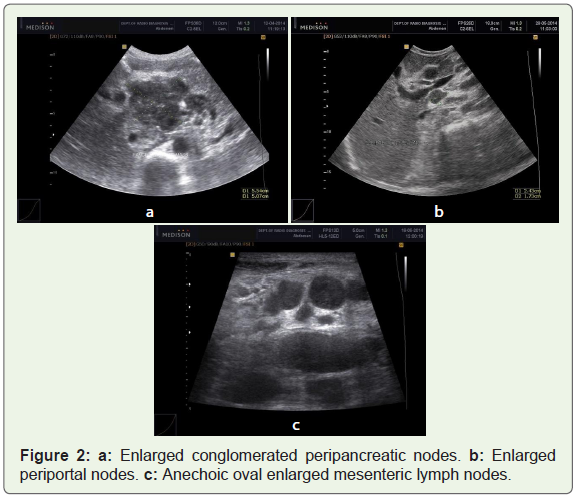
Splenomegalies found in 18 cases with or without hepatomegaly with or without enlarge nodes. In 6 cases there were abscesses in splenic parenchyma (Figure 3a and b, 3c). In 5 cases abscesses were small 2-10 mm in size and they were multiple in most of cases, in one abscess was of size 18mm. Splenic parenchyma was homogenous. These microabscesses were mostly due to disseminated tuberculosis [6,7]. They were appreciated properly with high frequency probe as hypo/anechoic small nodules. The larger lesion was due to other opportunistic/fungal as correlated with lab reports.
These lesions can be differentiated with from splenic infiltration by lymphoma in which appearance is more hetrogenous and sometimes cystic [1]. Splenomegaly was found associated with other abdominal findings like enlarge lymph nodes, ascites and hepatomegaly etc.
Ascites was found in 12 cases; in 6 cases it was associated with septations.
Ascitic fluid was having low level echoes. Ascites is commonly seen in patients of tuberculosis it can be septated ascites or non septated [8]. In our study were having pleural effusion also. Hypoproteinemia is another common cause of ascites as these patients are immunocompromised.
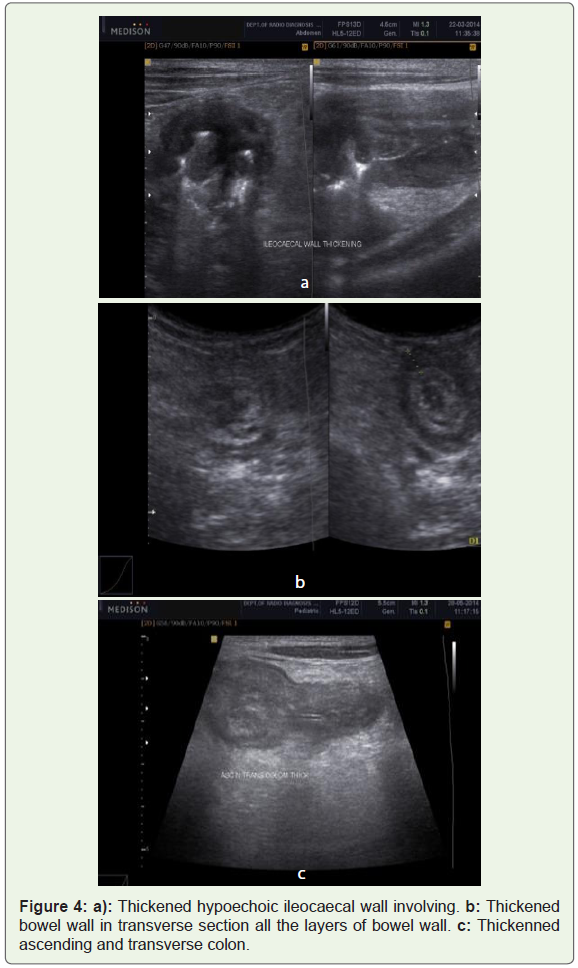
Bowel thickening the typical sonographic appearance of the normal bowel wall consists of five concentric, alternately echogenic and hypoechoic layers that we describe from the lumen outward [9]. A small echogenic layer is seen that reflects the superficial mucosal interface. The deep mucosa, including the muscularis mucosa, is seen as a second hyperechoic layer. A third hyperechoic layer is produced by the submucosa and the muscularis propria interface. The muscularis propria is seen as a fourth hypoechoic layer. Finally, the marginal interface to the serosa is seen as the fifth small hyperechoic layer. The average thickness of the normal gut wall i.e., 2 - 4 mm Bowel wall thickening can be tubercular Non tubercular [9]. There can be loss of haustration.
Most common cause of bowel involvement is tuberculosis. Risk of tuberculosis with CD4 count is less than 100 and with WHO stage 3 is significantly high. Impaired TH 1-type immune response in HIV/AIDS patient makes them prone for tuberculosis.
Tubercular abdominal manifestations can be enlarging nodes/adenitis, Ascites, Splenic abscesses, hepatitis, hepatomegaly renal abscesses bowel thickening and bowel obstruction tubo-ovarian masses and salpingitis [10]. Ascites may be associated with incomplete and complete septations.
Here we have found 4 cases of bowel thickening having tubercular etiology. Bowel thickening of terminal ileum, caecum and IC junction was found in 4 cases with fat stranding and enlarges lymph nodes (Figure 4a and 4b). It was long segment involvement of all the 5 layers of bowel with asymmetrical and circumferential thickening (Figure 1b). In the case of NHL it was short segment involvement of small bowelileum and IC junction with thickened all layers of bowel appearing hypoechoic. In this case there was thickening of ascending colon and transverse colon also as shown in Figure 4c. May be it was reactive thickening or due to some other opportunistic infection associated. As mentioned in literature in CMV infection bowel may be thickened in the region of ascending colon and caecum [9]. Other Associated findings were Hepatosplenomegaly and enlarge lymph nodes.
Reactive bowel thickening is also seen in HIV patients due to hypoproteinemia which is often remains underreported.
Non tubercular causes of bowel thickening are inflammatory response or could be due to HIV acquired neoplasia. There is large association with falling CD4 count. Tumors affecting HIV pts can be classified ad AIDS Defining Cancers ADC and NON AIDS Defining Cancers. AIDS Defining cancers are NHL, Kaposi sarcoma, hepatocellular carcinoma and Cervical Cancers. Non AIDS defining cancers are Lung and Breast cancers [1].
NHL associated with AIDS bears poor prognosis. It may involve several organs in abdomen like spleen, liver, kidneys and retro and intraperitoneal nodes. In Liver and spleen NHL manifest as multiple hypo or hypoechoic masses. NHL has some male predominance.
CD4 count can be correlated as [8] -
<350 cells /micron L -Kaposi Sarcoma,
<200 Cells /micron L-NHL
<100 cells /micron L -C M V Infection
Kaposi Sarcoma may involve small and large intestine, stomach, liver or genitourinary system. Though we could make out changes in bowel as described still CT can better delineate bowel pathologies.
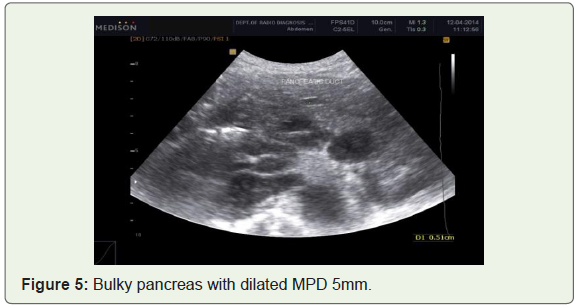
There can be pancreaticobiliary manifestations in patients of HIV such as GB wall thickening, bulky pancreas dilated MPD [11]. Gall Bladder pathology like thickened GB wall was found in 4 cases. In two of them it was acalculous cholecystitis and in another two there were gall bladder calculi. Though GB calculus are not so common in HIV patients.
Bulky Pancreas found in Two cases in one there was dilated MPD as 5mm (Figure 5). In the second case of bulky pancreas, there was increased AP diameter of 4 and body 3.2cms. There were enlarged peri pancreatic nodes.
There were two case of Cervicitis with fluid in POD. In one there were nabothian cysts also.
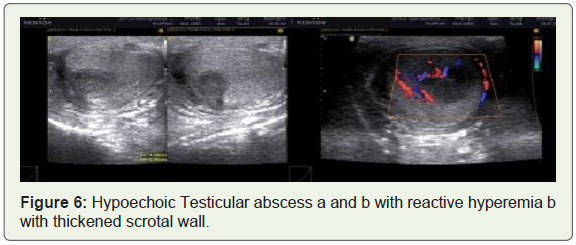
Two cases were of testicular abscess having other abdominal findings of enlarge retroperitoneal nodes also. Presented with hypoechoic area in testicular parenchyma with thickened wall of scrotal wall (Figure 6). There was hyperemia in surrounding parenchyma of testis. In one case there was thickened spermatic cord as well. Inguinal lymph nodes were enlarged in both cases along with abdominal nodes. One of them diagnosed as of tubercular etiology. Another was undetermined.
Renal findings in HIV patients are diverse such as Medical renal disease, Pyelonephritis or focal renal masses [12,13]. We could find two cases with renal findings. In our study most common presentation was Renomegaly with increased echogenicity of both cortex and medulla consistent with renal parenchymal disease. There were increased creatinine and urea levels [14].
There can be focal masses in renal parenchyma in cases of abscess long with nephromegaly. Lymphoma may show diffuse bulky kidneys [9,10].
One patient showed pyelonephritis with reduced parenchymal echogenicity. Low level echoes were seen in pelvicalyceal system along with thickened urinary bladder wall > 6mm and moving echoes s/o cystitis.
Conclusion
AIDS is multisystem disease but its demographic and clinical pattern remains same globally. USG is optimally suited for its clinical management especially in developing countries like India. Results of sonographically evaluated cases of abdominal findings are comparable to other diagnostic modalities like CT scan. The ease of availability, diagnostic accuracy of USG and its affordable cost and interventional and follow up advantages makes USG first choice of investigation for evaluation of abdominal findings. Clinico-pathological correlations can further increase its diagnostic accuracy.
Future prospective
1. Applying tele-USG for diagnosis at remote places in HIV positive high prevalence areas. 2. Better disease characterization using advances in USG technique.
Tissue elastography can help distinguishing tumors such as Kaposi Sarcoma and Lymphoma from other masses such as T.B and Pyogenic abscesses. This can reduce unnecessary biopsies and increase yield for positive histologies.
References
- Gosink BB, Leymaster CE (1981) Ultrasonic determination of hepatomegaly. J Clin Ultrasound 9: 37-44.
- Childs JT, Esterman AJ, Thoirs KA, Tuner RC (2016) Ultrasound in the assessment of hepatomegaly: A simple technique to determine an enlarged liver using reliable and valid measurements. Sonography 3: 47-52.
- Uygur-Bayramicli O, Dabak G, Dabak R (2003) A clinical dilemma: abdominal tuberculosis. World J Gastroenterol 9: 1098-1101.
- Lodengo H, Schoub B, Ally R, Kairu S, Segal I (2000) Hepatitis B and C virus infections and liver function in AIDS patients at Chris Hani Baragwanath Hospital, Johannesburg. East Afr Med J 77: 13-15.
- Geoffray A, Binet A, Cassuto JP, Dujardin Coussement A (1991) Sonongraphy of abdominal adenopathies in patients with HIV positive serology. In: Trotot PM (edn.) Imaging of AIDS. PP: 189-194.
- Murray JG, Patel MD, Lee S, Sandhu JS, Feldstein VA (1995) Microabscesses of the liver and spleen in AIDS: detection with 5-MHz sonography. Radiology 197: 723-727.
- Monill-Serra JM, Martinez-Noguera A, Montserrat E, Maideu J, Sabaté JM (1997) Abdominal ultrasound findings of disseminated tuberculosis in AIDS. J Clin Ultrasound 25: 1-6.
- Renn A, Kazmi F, Khan N, Rawal R, O’Boyle E (2017) The HIV manifestations within the gastrointestinal tract: A pictorial review. S Afr J Radiol 21: 1233.
- Sokolina I, Reshetnikov M, Sinitsyn M, Zuyzya J, Bormotov B (2017) Bowel disease in patients with HIV-positive patients: evaluation with CT. Electronic online presentation ECR 2017 / C-1501.
- Kawooya MG (2013) Abdominal ultrasound findings in HIV with tuberculosis. Imaging Med 5: 265-274.
- Miller FH, Gore RM, Nemcek AA Jr, Fitzgerald SW (1996) Pancreaticobiliary manifestations of AIDS. AJR Am J Roentgenol 166: 1269-1274.
- Frassetto L, Schoenfeld PY, Humphreys MH (1991) Increasing incidence of human immunodeficiency virus-associated nephropathy at San Francisco General Hospital. Am J Kidney Dis 18: 655-659.
- Schaffer RM, Schwartz GE, Becker JA, Rao TK, Shih YH (1984) Renal ultrasound in acquired immune deficiency syndrome. Radiology 153: 511-513.
- Anjana T, Trivedi A, Panchal M, Jethva M, Yadav M (2015) Abdominal ultrasonography findings in HV infected patients. Sch J App Med Sci 3: 504-507.