Research Article
Evaluation of Scrotal Pathologies by High-Resolution Ultrasound and Color Doppler
Sharma M1, Arora N2*, Sharma S3, Gupta AK4 and Mamta5
1S N Medical College, India
2Metro Heart Institute FaridabadFormerly resident S NMC, India
3V A Hospital West Palm Florida, USA
4UP University of Medical Sciences, India
5S N Medical College, India
Corresponding author: Arora N, Diagnostic Radiology, Metro Heart Institute FaridabadFormerly resident S NMC, India, E-mail: nitish1209@gmail.com
Citation: Sharma M, Arora N, Sharma S, Gupta AK and Mamta. Evaluation of Scrotal Pathologies by High-Resolution Ultrasound and Color Doppler. Indian J Appl Radiol. 2018;4(1): 122.
Copyright ©2018 Sharma M, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Applied Radiology | Volume: 4, Issue: 1
Submission: 23/05/2018; Accepted: 25/06/2018; Published: 29/06/2018
Abstract
Based on physical examination alone it is difficult to make clinical diagnosis accurately of scrotal pathologies. In this study we have studied 74 patients who presented with scrotal swelling or pain or both or with mass lesion in the surgery department and were referred to Radiodiagnosis department for USG from Feb 2011 to August 2012. These patients were evaluated with High-Resolution USG (HRUS) and Colour Doppler USG (CDUS) whenever needed. Differentiation of testicular-extratesticular lesion, cystic-solid lesions, acute inflammatory pathology or torsion of testis, Hernia-mass lesion is made easy and is of great diagnostic value by USG. The localization of ectopic /undescended testis is also done with USG.
In this study, Final diagnosis was Extratesticular fluid collection in 14 cases, Acute inflammation (orchitis as well as epididymitis) in 16 cases, Chronic inflammation in 6 cases, Varicocele in 10 cases, Scrotal Hernias in 7 cases, Testicular tumor in 2 cases, Undescended testis in 2 cases, Torsion testis in 3 cases, Extra testicular abscess in 2 cases, Epididymal cyst in 4 cases, Spermatocele in 2 cases, Hematocele in 2 cases, Pyocele in 2 cases, Testicular infarct in 1 case and Fournier’s gangrene in 1 case.
Keywords: HRUS; CDUS; Scrotal pathology
Introduction
A wide variety of disease process of scrotum manifest with pain or swelling or both and sometimes with mass. Prompt diagnosis is required to differentiate surgically correctable lesions from the lesions which can be corrected medically. To differentiate these processes with high-resolution ultrasound and Color Doppler Ultrasonography helps a lot.
Miskin, et al. for the first time described the use of scrotal ultrasonography in the assessment of testis. Since then lots of work has been done in evaluation of pathological conditions by USG [1].
A sudden onset of pain in the scrotum may be due to very serious cause such as Torsion of testis or Epididymitis. Torsion may need surgical intervention while epididymitis needs an antibiotic course. If left untreated torsion may lead to permanent damage to testis and if it is inflammatory cause it may lead to abscess formation [2,3].
In patients with scrotal mass, we can determine sonographically whether the mass is Intratesticular or Extratesticular. Also, nature of mass can be well ascertained whether it is cystic or solid or complex [4].
Collection of fluid and abnormalities of blood vessels which appear as scrotal masses can be well evaluated by USG. Following scrotal trauma surgery is needed to salvage testis. Use of Colour Doppler USG (CDUS) and Pulse Doppler sonography gives us information regarding morphology and perfusion [5]. CDUS is the first and initial technique in place of radionuclide imaging in the assessment of acute testicular torsion. Most common indication for Doppler Sonography is acute testicular torsion, scrotal trauma, undescended testis, Inflammation, and Infertility [6].
Materials and Methods
The group under study comprised of 74 patients of all age group both indoor and outdoor mostly referred to surgery department.
Method
Sonography equipment used was Sono Ace 8000 Samsung Medison using high-frequency probes 5-12 MHZ linear array transducer and also 3-7 MHZ in case of large scrotal swelling whenever needed.
Technique
Patients were asked to lie supine with legs slightly separated. A towel sling is placed beneath the scrotum for support. Penis was elevated onto the anterior abdominal wall and was covered by a drape. The gel was applied to the scrotum inadequate amount to avoid pressure and pain and served as the coupling agent. Scrotum was scanned from an anterior, lateral and posterior wall in longitudinal and transverse planes both. The examination was continued further to examine groin region. To see varicocele patients were examined in supine and erect posture with Valsalva maneuver. Scrotal masses were imaged in multiple planes and documented. Comparison with contralateral testis was helpful to demonstrate subtle changes in echotexture.
Color Doppler was done to depict flow in vessels. The testicular artery, capsular arteries, intratesticular vessels, cremasteric vessels were identified whenever possible. Power Doppler was applied whenever needed, PRF was kept low, the color window was small and color gain just below that which induced background noise. The comparison was made with normal side. Sonographic parameters studied in each case were -
1. Scrotal wall thickening.
2. The position of the testis, Size of the testis in transverse, AP, Superior-Inferior measurement.
3. Echotexture of testis.
4. Position, size, and echotexture of Epididymis.
5. Fluid collection in scrotal sac and its characteristics.
6. Inguinoscrotal region for varicocele or a hernia.
7. Vascularity of lesion was evaluated with both color Doppler and power Doppler.
Findings on CDUS evaluated as follows -
Grade 0 - No Doppler signal in evaluated scrotal mass or lesion.
Grade 1 - Spotty Doppler signal, < 2 vascular signal per 10mm.
Grade 2 - Scattered Doppler signal.
Grade 3 - Continuous flow uninterrupted vessel >25 mm inlength.
LAB investigation - Like urine routine Microscopy, Culture, ESR and ELSA for tuberculosis. Finally, collected data was analyzed to arrive at a definite diagnosis. Ultrasound findings were correlated with clinical findings and blood picture. Follow up was done in most cases.
Observations
The present study was conducted in Department of S.N Medical College Agra from Feb 2011-August 2012. A total of 74 patients with clinical symptoms related to scrotal pathology, referred from surgery were evaluated with high-resolution sonography.
Age distribution of 74 patients was -1-10 yrs -5 cases, 11-20yrs-12 cases, 21-30yrs -18 cases, 31-40yrs -20 cases, 41-50yrs- 8 cases, 51-60yrs -8cases, 61-70 yrs- 3 cases. Majority of patients were between 21-40 yrs (51.4%) and predominant group in the study was 31-40 yrs comprising of 20 patients (27.1%)(Table 1).
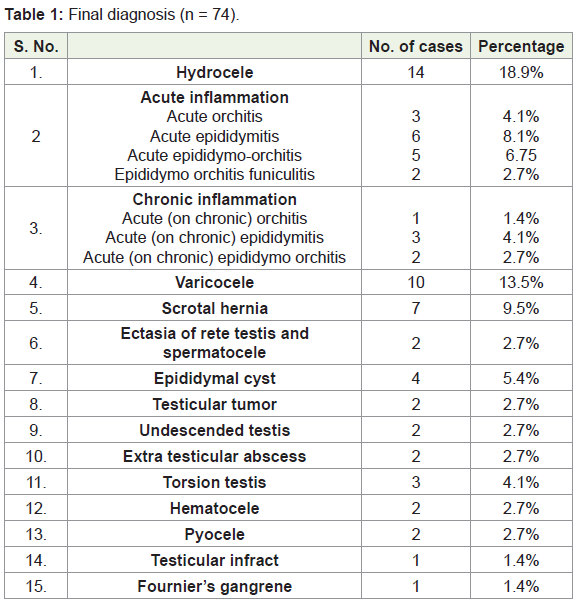
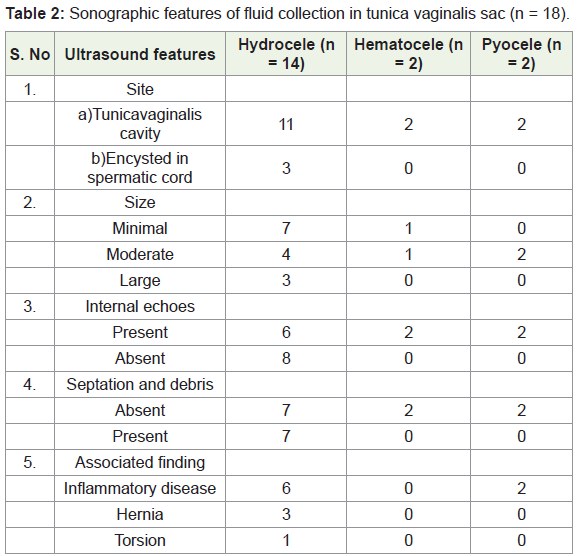
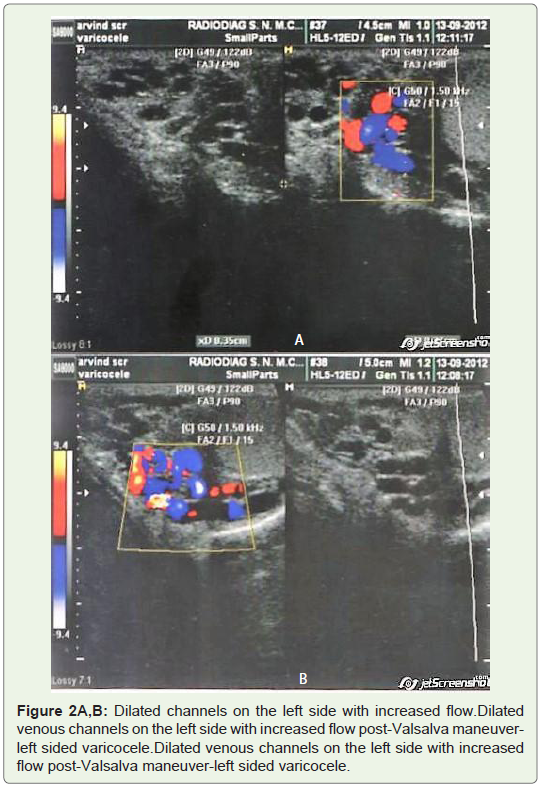
Fluid collection was the commonest abnormality detected on sonography. Hydrocele was seen in 14 (18.9%) cases and was the most frequent fluid collection. Most common type of hydrocele was the one with the fluid being confined to the tunica vaginalis cavity. Focal anechoic collection superior to the testis and epididymis, suggestive of encysted hydrocele of spermatic cord was noted in 3 cases (Table 2, Figure 1 and Figure 2).
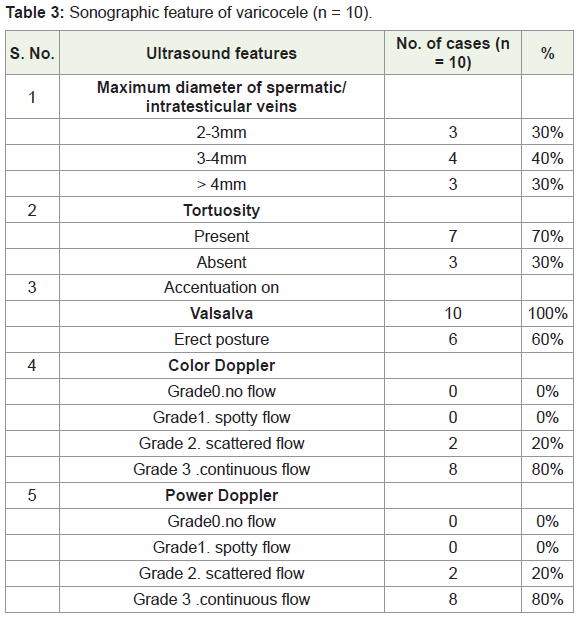
Varicocele comprised 13.5% of total no. of cases and 10% of the total pathological lesion. The maximum vessel diameter was more than 4mm in 3 cases (30%) in erect posture while tortuosity of vessels noted in 7 cases (70%). All cases demonstrated accentuation on Valsalva maneuver and on imaging erect posture (Table 3-5, Figure 2A,B).
Discussion
The present study was undertaken to evaluate the role of highresolution sonography, color flow index and power Doppler in the evaluation of scrotal pathology. A total of 74 patients from all age groups with signs and symptoms related to scrotal disease have been included in this study.
There were 100 various sonographic findings in total in these patients. Out of which 76.3% were extratesticular and 23.6% were intratesticular in origin. There was some overlap as both intra and extra testicular findings were found.
Age distribution
Majority of patients were between 21-40 yrs. Predominant age group was between 31-40 yrs as they face repeated trauma. Both inflammatory and neoplastic disease was more common in this age group.
Hydrocele
Fluid collection was commonest finding detected on USG. Hydrocele was seen in 14 cases and was subsequently proved on aspirate and cytology. Thus it was 100% accurately diagnosed on USG. Most commonly fluid was confined to tunica vaginalis. Fluid above the testis or epididymis was noted in 10% cases s/o encysted hydrocele. Two cases of hematocele were diagnosed which showed fluid with internal echoes both cases were referred with the history of trauma.
Acute inflammation
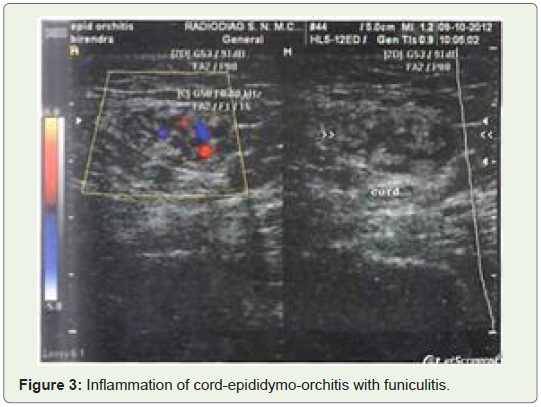
In the present study 16 (21.6%) patients were of acute inflammation. Maximum was 21-40yrs old and were sexually active. Among them 11 cases were of orchitis, 13 were epididymitis and two were epididymoorchitis. 8 patients showed increased size, 9 pts showed decreased echogenicity of the involved testis. To differentiate this from torsion, we did Doppler sonography. In cases of inflammation, we found hyperemia (Figure 3). In Epididymitis there was enlargement of epididymis with altered echotexture and inhomogeneity. Head was usually involved; Spermatic cord involvement is seen in 2 patients [7,8].
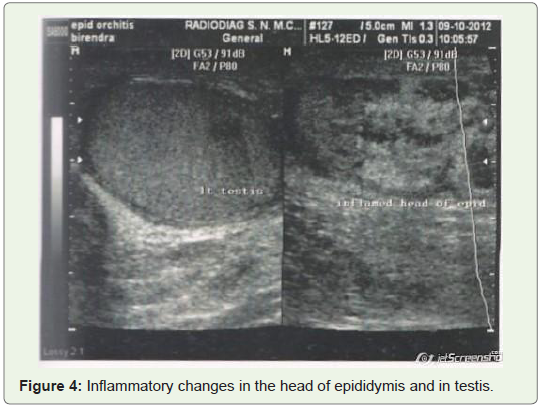
Color Doppler has been shown to be very sensitive in detecting hyperemia of Testis or Epididymis or both. Hyperemia may be the only finding without grayscale abnormalities. Following treatment Color Doppler shows resolution of hyperemia the Resistive index may decrease (Figure 4).
Spectral analysis of 7 out of 11 cases of Acute Orchitis with or without Epididymis involvement showed PSV > 15 cms/sec with a diagnostic accuracy of 90% for orchitis and 93% for Epididymitis. RI less than 0.5 were seen in 7 out of 11 cases of Orchitis and 9 out of 13 cases of Epididymitis [8].
Chronic inflammation
6 patients were with chronic inflammation of scrotal sac, the majority were in the age group 21 - 40 yrs. At final diagnosis, testes were involved in 3 cases and Epididymitis in 5 cases out of which one case of Orchitis and 4 cases of Epididymitis was tubercular in nature.
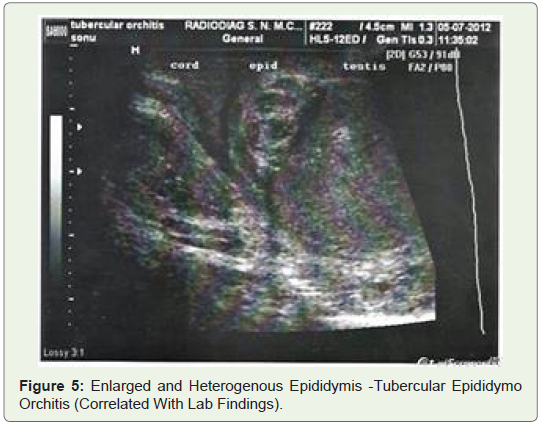
In the majority of Chronic Inflammatory conditions, testis/epididymis was hypoechoic with heterogeneity. In Tubercular cases, small hypoechoic nodules and tiny calcifications were seen. Complications of epididymal-orchitis mainly include Abscess formation, Infertility, Pyocele, Infraction, and Atrophy (Figure 5).
Varicocele
In the present study 10 (13.5%) cases of varicocele were included. All of these were correctly diagnosed. On grayscale varicocele was seen as multiple hypoechoic serpiginous and tubular structures larger than 2mm in diameter seen superior or lateral to the testis. Color Doppler depicted blood flow in these tubular channels. These findings were in accordance with Dogra, et al. All cases showed accentuation on Valsalva maneuver. On spectral analysis, these vessels showed venous flow pattern.
Scrotal hernia
7 cases of a scrotal hernia were noted in the present study. Omentum was seen herniating into the inguinoscrotal region in 2 cases while bowel loops in 5 cases. In our study sonography revealed a highly echogenic mass separated from testis in the scrotal sac which was Omentum. In case of Enterocele, multiple small bowel loops with bowel contents and peristalsis were observed.
Testicular Cyst and Epididymal Cyst and Spermatocele
In the present study 2 cases of the testicular cyst and 4 cases of the epididymal cyst and 2 cases of spermatocele were identified. The cyst was seen as anechoic structures with posterior acoustic enhancement. Both epididymal cyst and spermatocele are found in the head of the epididymis. Septations are found n 50% cases of spermatocele which are not seen in the epididymal cyst. However, these conditions could not be reliably differentiated on USG alone [9,10].
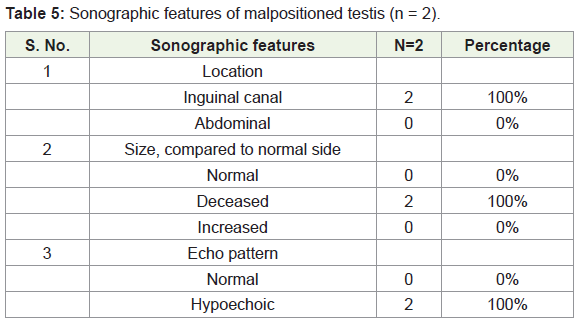
Malpositioned Testis
The incidence of undescended testis was 2.7% in our study. Both patients had unilateral undescended testis. The location of undescended testis was in the inguinal region in both patients. Both were proved histopathologically as Seminomas. In one patient it was within the inguinal region and in another, it was near the superficial inguinal ring. MRI is highly accurate ~93% in locating undescended testis [11].
Testicular tumors
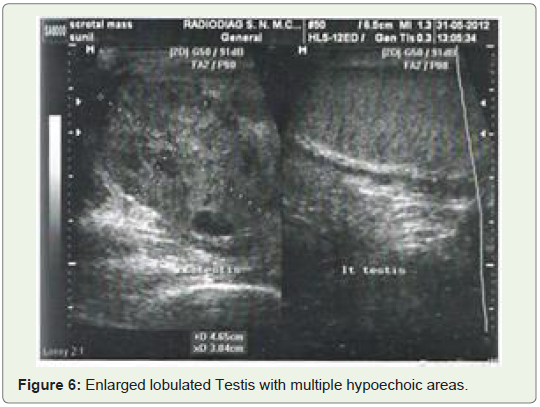
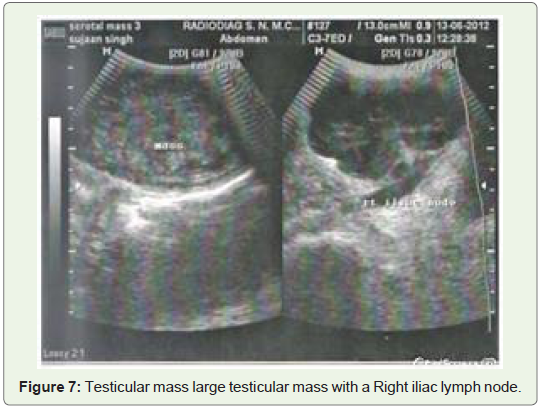
In the present study testicular tumors were found in two cases. Both the cases were between 21-40 yrs. They were having large masses of relatively hypoechogenecity and lesions were well-defined. Both were proved histopathologically as Seminomas (Figure 6 and Figure 7).
Grantham JG, et al. 1995 reported that testicular tumors represent 1-2% malignancy in males. Patients usually present with a painless mass. Seminomas are the most common type of non-mixed testicular tumor. Nachtscheim, et al. 1983 reviewed 17 patients with testicular tumors. Two categories were identified. Seminomas and Lymphomas appeared hypoechoic and homogenous. They had sharply demarcated borders. While NSGCT were of lower echogenicity appeared to have cystic spaces, acoustic shadowing, and irregular borders. Other tumors such as Teratomas, Choriocarcinoma, Adenomatous tumors, Fibromas, Leiomyoma are seen in the descending order. Metastasis in Testis is not common.
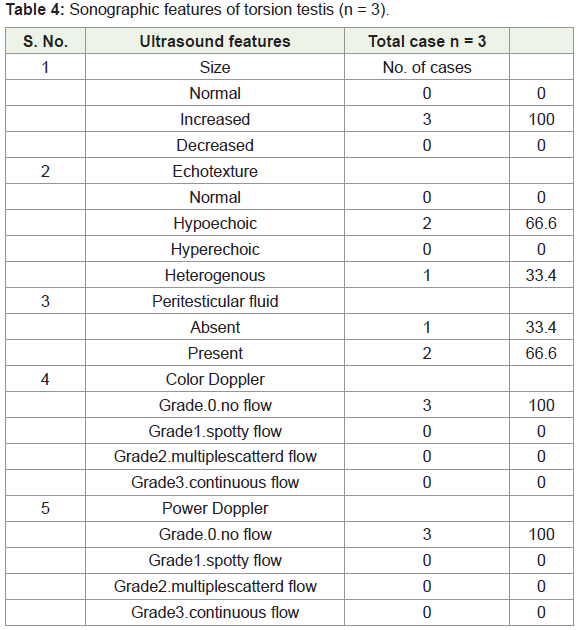
Testicular Torsion
In the present study 3 cases of testicular torsion were detected. Testicular Torsion occurs when spermatic cord is twisted (Allan, 1996). The predisposing condition is the presence of a short segment of mesenteric attachment, the bell clapper deformity. Torsion occurs most commonly in 12 -18 years of age. It is extravaginal when entire testis, epididymis and tunica vaginalis twist in a vertical axis on spermatic cord or intravaginal. Testicular salvage is possible in 80-100% of cases if surgery is done within 5-6 hrs. Traubici J, et al. 2003 studied 30 patients of torsion. Based on their study sonographic appearance of testicular torsion can be
1. Acute: Enlarged Testis, heterogenous echotexture no detectable flow and hydrocele.
2. Subacute: Normal size testis, heterogenous echotexture, small hydrocele.
3. Chronic: Small testis, small amount of testicular tissue left, areas of increased echogenicity and no hydrocele.
Dogra, et al. gave Color flow Doppler patterns in testicular torsion [12] -
1. Absent arterial and venous flow.
2. Increased RI on affected side decreased or reversed diastolic flow.
3. Decreased flow velocity.
4. Low amplitude flow on symptomatic side.
Testicular microlithiasis:
In our study testicular microlithiasis found in 1.4% cases. They are multiple 1-2mm sizes diffusely scattered hyperechoic foci within testicular parenchyma. If they are found annual follow up of USG is recommended in view of its association with neoplasia.
Summary and Conclusion
This study was undertaken to evaluate scrotal Pathologies by High-resolution grey scale sonography, CDFI, and PD in the evaluation of scrotal pathology.
A total of 74 patients from all age group with signs of symptoms related to scrotal disease were evaluated. All the patients were properly followed up sonographically /medically /surgically /pathologically as per indication.
Idiopathic hydrocele was most common scrotal pathology it featured as anechoic fluid in tunica vaginalis and it was correctly diagnosed on a grey scale. Extratesticular fluid following trauma and infection depicted septations.
In patients of acute inflammation, Doppler sonography showed increased blood flow in affected epididymis and testis and thus showed 100% accuracy. The commonest pattern was enlarged testis or epididymis with altered echotexture. PD was more sensitive than color Doppler. PSV > 15cms /sec and RI less than 0.5 were complementary to diagnosis.
In the cases of suspected Torsion of testis /acute inflammation, it is difficult to differentiate two by grey scale imaging. However, CDFI in symptomatic testis showed the absence of vascular signals in cases of Torsion of Testis.
Among the cases of chronic inflammation tubercular epididymoorchitis was most common. Epididymis was more commonly involved as compared to the testis. The tail of epididymis suffered more than a body and showed heterogeneous echotexture.
In cases of Varicocele, Grayscale was 80% sensitive. It failed to diagnose subclinical varicocele in infertile males in which venous diameter of pampiniform plexus was 2-3mm. However Color Doppler and pulse Doppler accurately diagnosed in all cases (100% sensitivity).
The undescended testis was noted in two cases and in both cases testis was located in inguinal canal and condition was unilateral. The testis was hypoechoic and small in size. Of the 7 cases of a scrotal hernia, Omentocele was seen in 2 cases and Enterocele in 5 cases.
In our study, most of the observations and results matched earlier studies. However, there were few results which did not match with earlier studies. This may be due to the smaller sample size of our study.
To summarize an excellent correlation was seen in the diagnosis of scrotal lesions between sonography (Grayscale, CDFI and PD) and histopathology /surgery /treatment response.
Sonography, both Grayscale and Color Doppler were found to be 93.33% sensitive in the diagnosis of Scrotal Pathology. The present study concludes that High-Resolution USG along with Color Doppler imaging and Power Doppler should be used as the first imaging modality in the evaluation of Scrotal Pathology.
References
- Miskin M, Bain J (1974) B mode ultrasonic examination of testis. J Clin Ultrasound 2: 307-311.
- Leopold GR, Woo VL, Scheible FW, Nachtsheim D, Gosink BB (1979) High-resolution ultrasonography of scrotal pathology. Radiology 131: 719-722.
- Arger PH, Thurner S (1995) Diagnostic capabilities of high resolution scrotal sonography. J ultrasound Med 4: 3-10.
- Carroll BA, Gross DM (1983) High-frequency scrotal sonography. AJR Am J Roentgenol 140: 511-515.
- Murry M (1990) Color Doppler sonography of scrotal masses. AJR 114: 649-655.
- Robert A, Mecorach, et al. (1994) Color Doppler ultrasound evaluation in acute scrotal disease. AJR 163: 548-554.
- Horstman WG, Middleton WD, Melson GL, Siegel BA (1991) Color Doppler ultrasound of the scrotum. RadioGraphics 11: 941-958.
- Brown JM, Hammers LW, Barton JW, Holland CK, Scoutt LM, et al. (1995) Quantitative Doppler assessment of acute scrotal inflammation. Radiology 197: 427-431.
- Watanabe Y, Dhoke M, Ohkubo K, Ishimori T, Amoh Y (2000) Scrotal disorders: Evaluation of testicular enhancement patterns at dynamic contrast-enhanced subtraction MR imaging. Radiology 217: 219-227.
- Sidhu PS (1999) Clinical and imaging features of testicular torsion: role of ultrasound. Clin Radiol 54: 343-352.
- Woodward PJ, Sohaey R, O’Donoghue MJ, Green DE (2002) From the archives of the AFIP: tumors and tumorlike lesions of the testis: radiologic-pathologic correlation. Radiographics 22: 189-216.
- Vikram S, Dogra (2004) Torsion and beyond. J ultrasound in Medicine 23: 1073.