Images Section
Cervical Cord Pseudomeningocele: Unusual Late Complication of Spine Surgery
Muhammad Taimur Malik1* and Sunil Jeph2*
1Department of Neurology, Geisinger Medical Center, Danville, USA
2Department of Radiology, Geisinger Medical Center, Danville, USA
Corresponding author: Muhammad Taimur Malik, Department of Neurology , Geisinger Medical Center, 100 North Academy Avenue, Danville, PA 17822, USA, Tel: 781-333-8547; E-mail: mamalik@geisinger.edu; Sunil Jeph, Department of Radiology, Geisinger Medical Center, 100 North Academy Avenue, Danville, PA 17822, USA, Tel: 914-307-8473; E-mail: sjeph@geisinger.edu
Citation: Malik MT, Jeph S. Cervical Cord Pseudomeningocele: Unusual Late Complication of Spine Surgery. Indian J Appl Radiol. 2017;3(1): 118.
Copyright © 2017 Malik MT, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Applied Radiology | Volume: 3, Issue: 1
Submission: 26/10/2017; Accepted: 17/11/2017; Published: 20/11/2017
Keywords: Pseudomeningocele; Cervical cord stenosis; Post-operative
Case Presentation
66-year-old man presented with one-day history of left arm numbness, which spontaneously resolved. The numbness initially started in his hand and later ascended to involve proximal muscles. Past medical history was significant for cervical spine fusion surgery (C4-C6) 40 years ago, complicated by epidural hematoma with emergent evacuation. He has been asymptomatic for last 40 years. Vitals were stable, neurological exam showed some baseline weakness of 4/5 in the right deltoid and triceps with no other pertinent neurological findings. Patient was admitted for TIA work up. MRI brain and TTE were unremarkable. While MRI cervical spine revealed spinal cord edema from C2 to C6 vertebra levels with severe spinal canal stenosis caused by dorsal fluid collection extending from C3-C6 as shown in Figure 1. CT myelogram was consistent with Pseuduomeningocele as shown in the Figure 2. Pseudomeningoceles are extradural collections of cerebrospinal fluid (CSF) that communicate with subarachnoid space and are caused by dural breach secondary to spinal cord surgeries and trauma. Clinical symptoms depend on the location and chronicity of the lesions as our patient had minimal symptoms from such an extensive cord compression[1]. The treatment depends upon the extent of clinical symptoms and usually involve conservative management to invasive surgical repair.

Figure 1: T2 weighted MRI sagittal (A) and axial (B) images of the cervical spine show fluid signal in the pseudomeningocele pouch causing severe spinal cord compression (arrow) resulting in edema in the proximal and distal spinal cord.
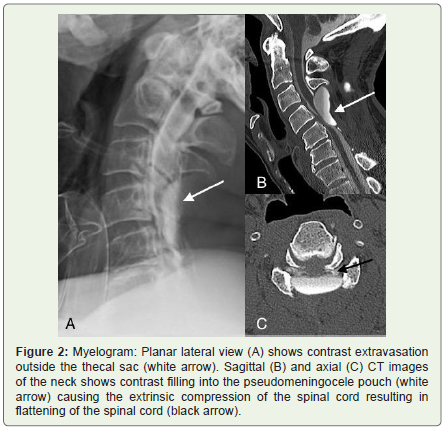
Figure 2: Myelogram: Planar lateral view (A) shows contrast extravasation outside the thecal sac (white arrow). Sagittal (B) and axial (C) CT images of the neck shows contrast filling into the pseudomeningocele pouch (white arrow) causing the extrinsic compression of the spinal cord resulting in flattening of the spinal cord (black arrow).