Case Report
CT & MRI Findings in a Rare Case of Total Fat Replacement of Pancreas
Dwivedi MK1*, Diwakar RK2 and Govindwar A3
1Assistant Professor, Department of Radio-diagnosis, Chandulal Chandrakar Memorial Medical College, Kachandur, Chhattisgarh, India
2Associate Professor, Department of Radio-diagnosis, Chandulal Chandrakar Memorial Medical College, Kachandur, Chhattisgarh, India
3Senior Resident, Department of Radio-diagnosis, Chandulal Chandrakar Memorial Medical College, Kachandur, Chhattisgarh, India
Corresponding author: Dwivedi MK, Assistant Professor, Department of Radio-diagnosis, Chandulal Chandrakar Memorial Medical College, Kachandur, Chhattisgarh-490024, India; Tel: 9407983539; E-mail: mahendra_van@yahoomail.com
Citation: Dwivedi MK, Diwakar RK, Govindwar A. CT & MRI Findings in a Rare Case of Total Fat Replacement of Pancreas. Indian J Appl Radiol. 2017;3(1): 116.
Copyright © 2017 Dwivedi MK, et al.This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Applied Radiology | Volume: 3, Issue: 1
Submission: 14/10/2017; Accepted: 13/11/2017; Published: 15/11/2017
Abstract
Total fat replacement of the pancreas is rare. Focal fatty replacement is the most common degenerative lesion of pancreas. Focal fatty deposits have no major clinical significance; however, extreme fat replacement may be associated with marked reduction in exocrine function of pancreas, resulting in malabsorption due to pancreatic enzyme insufficiency. We report CT & MRI findings in an incidental case of advanced pancreatic lipomatosis where the whole parenchyma is replaced by fat without exocrine or endocrine pancreatic dysfunction and the pancreatic duct is identified as a linear density.
Keywords: CT; Fatty infiltration; Fatty pancreas; Lipomatosis; MRI; Total fat replacement of pancreas
Introduction
Pancreatic lipomatosis also called fat replacement represents the most frequent benign pathologic condition of the adult pancreas [1]. Most cases remain asymptomatic and only some extreme degree of fat replacement may lead to exocrine pancreatic insufficiency. It is regarded as a normal finding in the obese and the elderly [2,3]. In the obese, it should be termed fat infiltration rather than fat replacement, since this condition is reversible on weight reduction. Uneven fat infiltration is more refractory to weight loss. The precise etiology remains unknown and may be multifactorial. The diagnosis is classically made by ultrasound, CT and MRI in the vast majority of cases.
Case Report
A female patient of 46 years with complaints of pain in abdomen off and on for the last one year was referred to imaging centre of our hospital for further investigation. The abdominal ultrasound done in some outside centre revealed no significant abnormal findings.
There was no history of jaundice, pruritus, pale stool, osmotic symptoms or any signs suggestive of pancreatitis/pancreatic cancer or malabsorption syndrome. Physical examination was unremarkable. Clinical biochemistry and labs yielded normal results. Stool fat content was 20 droplets/hpf. Pre-and postprandial blood sugar levels, serum amylase, lipase, total serum proteins, and albumin levels were within normal range that rules out the possibility of endocrine and exocrine deficiencies. Biomarkers for hepatitis were negative. The X-ray chest was normal.
CT was performed on GE FXI high speed single slice scanner with scan time of 1 second per slice which revealed total replacement of pancreatic tissue by fat attenuation substance having CT values of -117 HU.
NCECT and CECT revealed pancreatic duct and normal intrapancratic vessels; with normal pancreatic contour preserved and no evidence of pancreatic atrophy (Figures 1 and 2).
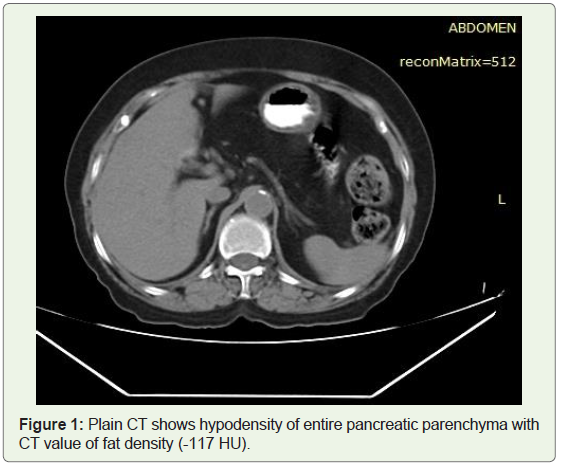
Figure 1: Plain CT shows hypodensity of entire pancreatic parenchyma with CT value of fat density (-117 HU).
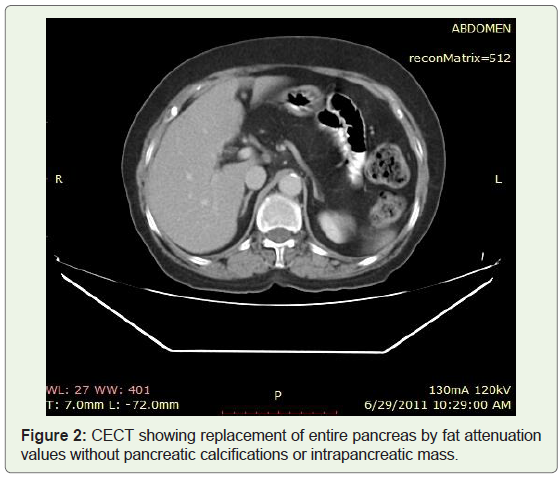
Figure 2: CECT showing replacement of entire pancreas by fat attenuation values without pancreatic calcifications or intrapancreatic mass.
MRI was done on 1.5 Tesla GE Signa Excite.
MRI Axial T2 weighted image revealed hyperintense pancreas; MRI AX SSFSE T2 FatSat image showed complete replacement of pancreas by fat; MRI Axial Lava sequence post contrast showed pancreatic duct without significant enhancement in pancreatic region (Figures 3-5).
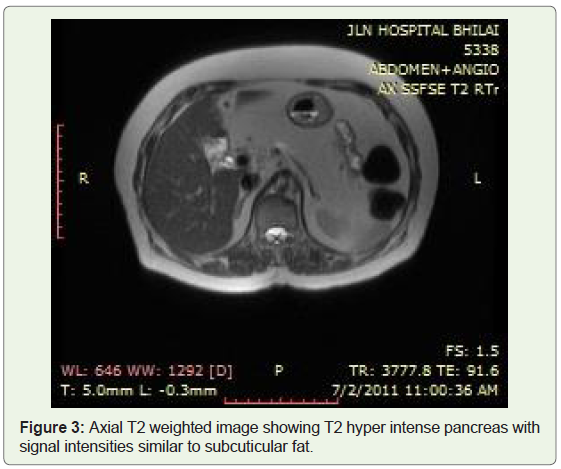
Figure 3: Axial T2 weighted image showing T2 hyper intense pancreas with signal intensities similar to subcuticular fat.
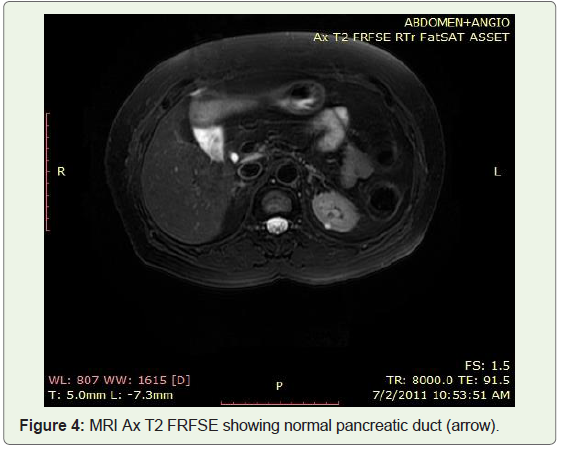
Figure 4: MRI Ax T2 FRFSE showing normal pancreatic duct (arrow)
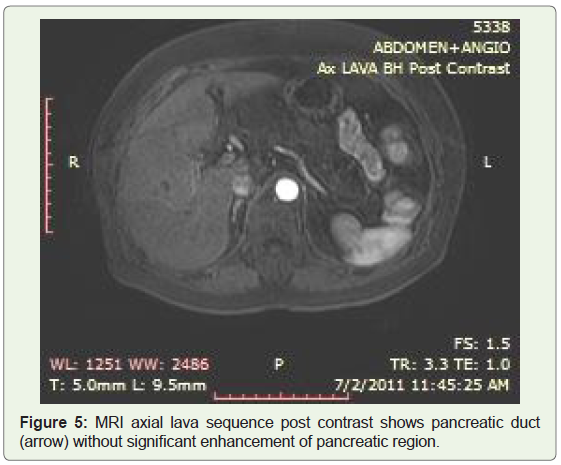
Figure 5: MRI axial lava sequence post contrast shows pancreatic duct (arrow) without significant enhancement of pancreatic region.
Discussion
Terminology
Accumulation of fat within pancreas (lipomatosis) and replacement of various portions of the pancreatic gland by fat (fat replacement) have been named with various synonyms: pancreatic lipomatosis, fatty replacement, fatty infiltration, fatty pancreas, lipomatous pseudohypertrophy, non-alcoholic fatty pancreatic disease and pancreatic steatosis [4]. These synonyms are sources of confusion.
On the basis of the various imaging findings, one could be inclined to use the term of “lipomatous infiltration” when the pancreatic glandular islands appear dissociated by fatty tissue or when the density (CT), echogenicity (ultrasound), or signal (MRI) are diffusely modified. When the pancreatic islands seem to have disappeared or been grossly replaced by fat, one might be more prone to prefer the vocable “fat replacement” [4,5].
The terms fat replacement and lipomatosis of the pancreas have been replaced by the simplified term fatty infiltration, or “FI”. It highlights that FI of the pancreas may be uniform, unevenly distributed, or confined to one region of the pancreas (focal FI) [6,7].
The fatty changes in pancreatic lipomatosis may be either focal or total in extent.
Subtypes: 1) even pancreatic lipomatosis 2) uneven pancreatic lipomatosis [8]
Classically, the different patterns of uneven Fatty Infiltration (FI) described by Matsumoto are commonly found during clinical CT imaging [9]:
The posterior pancreatic head (PPH) and uncinate process (UP) are spared from FI in type 1
FI involves all the head except a very small refractory focal area around the common bile duct in type 2
This case possibly belongs to type 2b fatty infiltration.
Nevertheless, there is a massive lack of significant histopathological studies to prove or disprove that lipomatosis and fat replacement of the pancreas are (i) distinctive entities, (ii) associated entities in variable proportions in a definite case, or (iii) expressions of the same disease.
Lipomatous Pseudohypertrophy (LPH) of the pancreas, a rare, specific, and distinct entity was first described by Hantelmann in 1931 as a disproportionate replacement of the entire pancreas with increasing amounts of adipose tissue and subsequent enlargement of the entire gland [10].
Etiology
The exact etiopathogenesis behind fatty replacement is not known; however, several predisposing factors suggested including systemic and local causes and its association with various syndromes has been enumerated below:
1) Systemic
2) Local
3) Syndromic associations
Pancreatic lipomatosis has been found associated with several diseases comprising diabetes mellitus, metabolic syndrome, acquired or hereditary pancreatitis, alcoholic hepatitis, cystic fibrosis [12], and condition comprising increasing age, body mass index or more precisely visceral fat index and use of steroid therapy. Numerous cases are associated with condition compromising the permeability of the pancreas ductal system such as intraductal calculus, pancreatic tumors [13], and congenital or experimental stenosis [14].
Total fatty replacement of pancreas is important for radiologists as it results in malabsorption due to pancreatic exocrine insufficiency [9].
Role & limitations of imaging modalities
The role of ultrasound in the diagnosis of pancreatic steatosis is very limited; first, because the overlying bowel gas causes obscuration of the pancreas and second, the fatty infiltration results in increased echogenicity of the pancreatic tissue making its differentiation difficult from normal retroperitoneal fat.
Cross-sectional imaging, namely, CT and MRI has an important role in the evaluation of pancreatic disease. CT is particularly useful in detecting specific etiologies, for example, pancreatic duct obstruction by the calculus or tumor.
Unenhanced CT has negative attenuation value of pancreatic tissue replaced by the fat, therefore can reliably diagnose diffuse fatty change involving the pancreas. However, focal fatty change cannot be diagnosed confidently with CT alone, as on post contrast images, the normal pancreatic parenchyma entrapped between fatty replacement area shows contrast enhancement simulating a true mass [15].
Chemical shift MRI has advantage over CT in confirming the presence of focal fatty replacement of the pancreas due to its ability to distinguish fat from other tissues and because of fat suppression techniques [16]. A characteristic loss of signal intensity on opposedphase T1-weighted gradient-echo image as compared with corresponding in-phase image confirms the presence of microscopic lipid within the focal pancreatic mass [17]. This histologic condition is, in general, not present in pancreatic cancer [18]. MRI sequences with fat suppression are also useful for the diagnosis of FI.
MRCP/ERCP demonstrates the status of pancreatic duct and the biliary tree. Selective pancreatic angiography is especially useful in differentiating pancreatic lipomatosis from dorsal agenesis by showing the pancreatic circulation [13].
Sijens PE et al. determined fat content of human liver, pancreasand kidneys using MR spectroscopy and a previously validated gradient echo magnetic resonance imaging method with Dixon’s two point technique [19].
Lipotoxic damage to organs
It has been hypothesized that in obesity and metabolic syndrome, ectopic fat causes lipotoxic damage to organs e.g. Liver (steatohepatitis and cirhhosis), pancreas ( beta-cell dysfunction) and lipotoxicity of the kidney [20-24]. They concluded that the role of lipid accumulation in the pathogenesis of renal disease, diabetes and metabolic disease in human should be reconsidered.
A correlation has been demonstrated that obese nondiabetic subjects have increased fat in the pancreas and lipomatosis of the pancreas reflects early events in the pathogenesis of diabetes [25,26].
Marked pancreatic lipomatosis with atrophy has been observed in adult patients secondary to pancreatic duct obstruction by calculi or carcinoma [27]. Under these circumstances, the obstructed pancreatic duct is stenotic rather than dilated, and typically has a smooth wall. Important differentials in case of stenotic pancreatic duct include dorsal agenesis of pancreas, pancreatic carcinoma and chronic pancreatitis [27].
Haunz and Baggenstoss reported fat replacement in the body and tail of pancreas in a clinical study of 80 cases of carcinoma head of pancreas [28].
Pancreatic lipomatosis with stenotic pancreatic duct, secondary to pancreatic head adenocarcinoma after neoadjuvant chemoradiotherapy has been reported by Makay et al. [29].
Pancreatic lipomatosis following chronic pancreatitis/carcinoma is focal or diffuse associated with parenchymal atrophy that manifests as exocrine and endocrine or only exocrine deficiency. In normal individuals, only 10% of parenchyma is sufficient for the maintenance of normal exocrine function [30].
Differential diagnosis includes pancreatic agenesis: pancreatic duct is preserved in pancreatic lipomatosis.
Conclusion
The echogenecity of pancreas gradually increases with age & obesity. When pancreas becomes very lipomatous and extremely hyperechoic, the performance of ultrasound in its diagnosis reduces drastically. Abdominal CT & MRI can be reliably used in diagnosis of total fat replacement and fatty infiltration of the pancreas and associated conditions.
References
- Patel S, Bellon EM, Haaga J, Park CH (1980) Fat replacement of the exocrine pancreas. AJR Am J Roentgenol 135: 843-845.
- Walters MN (1966) Adipose atrophy of the pancreas. J Pathol 92: 547-557.
- Dreilling DA, Eisbach P, Schaffner F, Schwartz IL (1962) The effect of restriction of protein and total calories on pancreatic function in obese patients. Gastroenterology 42: 686-690.
- Pezzilli R and Calculli L (2014) Pancreatic steatosis: Is it related to either obesity or diabetes mellitus? World J Diabetes 5: 415-419.
- Patel S, Bellon EM, Haaga J, Park CH (1980) Fat replacement of the exocrine pancreas. AJR Am J Roentgenol 135: 843-845.
- Ozbulbul NI, Yurdakul M, Tola M (2010) Does the visceral fat tissue show better correlation with the fatty replacement of the pancreas than with BMI? Eurasian J Med 42: 24-27.
- Yang DM, Kim HC, Ryu JK, Joo KR, Ahn KJ (2010) Sonographic appearance of focal fatty infiltration of the pancreas. J Clin Ultrasound 38: 45-47.
- Mortele KJ, Rocha TC, Streeter JL, Taylor AJ (2006) Multimodality imaging of pancreatic and biliary congenital anomalies. Radiographics 26: 715-731.
- Matsumoto S, Mori H, Miyake H, Takaki H, Maeda T, et al. (1995) Uneven fatty replacement of the pancreas: Evaluation with CT. Radiology 194: 453-458.
- Hantelmann W (1931) Fettsucht und Atrophie der Bauchspecicheldruse bei Jungendlichen. Virchows Arch 282: 630-642.
- Mendez-Uriburu L, Ahualli J, Mendez-Uriburu J, Mendez-Uriburu M, Fajre L, et al. (2004) CT appearances of intraabdominal and intrapelvic fatty lesions. AJR Am J Roentgenol 183: 933-943.
- Soyer P, Spelle L, Pelage JP, Dufresne AC, Rondeau Y, et al. (1999) Cystic fibrosis in adolescents and adults: Fatty replacement of the pancreas--CT evaluation and functional correlation. Radiology 210: 611-615.
- Baek SY, Lee SC, Kim MY, Lee MG, Cho KS, et al. (1992) CT findings of pancreas lipomatosis and associated diseases. J Korean Radiol Soc 28:749-753.
- Coulier B (1996) Hypoechogenic aspects of the ventral embryonic cephalic pancreas: A large prospective clinical study. J Belge Radiol 79: 120-124.
- Walters MN (1966) Adipose atrophy of the pancreas. J Pathol 92: 547-557.
- Kim HJ, Byun JH, Park SH, Shin YM, Kim PN, et al. (2007) Focal fatty replacement of the pancreas: Usefulness of chemical shift MRI. AJR Am J Roentgenol 188: 429-432.
- Anand R, Narula MK, Chaudhary V, Agrawal R (2011) Total pancreatic lipomatosis with malabsorption syndrome. Indian J Endocrinol Metab 15: 51-53.
- Unger RH (2003) Minireview: Weapons of lean body mass destruction: the role of ectopic lipids in the metabolic syndrome. Endocrinology 144: 5159-5165.
- Sijens PE, Edens MA, Bakker Stephan JL, Stolk RP (2010) MRI-determined fat content of human liver, pancreas and kidney. World L Gastroenterol 16: 1993-1998.
- Wahba IM, Mak RH (2007) Obesity and obesity-initiated metabolic syndrome: Mechanistic links to chronic kidney disease. Clin J Am Soc Nephrol 2: 550-562.
- Weinberg JM (2006) Lipotoxicity. Kidney Int 70: 1560-1566.
- Clark JM, Diehl AM (2003) Nonalcoholic fatty liver disease: An underrecognized cause of cryptogenic cirrhosis. JAMA. 289:3000-3004.
- Poitout V, Robertson RP (2008) Glucolipotoxicity: Fuel excess and beta-cell dysfunction. Endocr Rev 29: 351-366.
- Wahba IM, Mak RH (2007) Obesity and obesity-initiated metabolic syndrome: Mechanistic links to chronic kidney disease. Clin J Am Soc Nephrol 2: 550-562.
- Kovanlikaya A, Mittelman SD, Ward A, Geffner ME, Dorey F, et al. (2005) Obesity and fat quantification in lean tissues using three-point Dixon MR imaging. Pediatr Radiol 35: 601-607.
- Raeder H, Haldorsen IS, Ersland L, Gruner R, Taxt T, et al. (2007) Pancreatic lipomatosis is a structural marker in nondiabetic children with mutations in carboxyl-ester lipase. Diabetes 56: 444-449.
- Nakamura M, Katada N, Sakakibara A, Okumura N, Kato E, et al. (1979) Huge lipomatous pseudohypertrophy of the pancreas. Am J Gastroenterol 72: 171-174.
- Haunz EA, Baggenstoss AH (1950) Carcinoma of head of the pancreas. ArchPathol 49: 367-386.
- Makay O, Kazimi M, Aydin U, Nart D, Yilmaz F, et al. (2010) Fat replacement of the malignant pancreatic tissue after neoadjuvant therapy. Int J Clin Oncol 15: 88-92.
- Reddy OJ, Gafoor JA, Reddy GM, Prasad PO (2015) Total pancreatic lipomatosis: A rare presentation. J NTR Univ Health Sci 4: 272-274.