Research Article
Imaging of Osseous Lesions in Langerhans Cell Histiocytosis (LCH)
Sujata Patnaik1*, Yarlagadda Jyotsnarani2, Harsha Vardhana Kuruba Ramanjeneyulu3 and Susarla Ramamurti4
1Department of Radiology and Imageology, Additional Professor, Nizam’s Institute of Medical Sciences, Hyderabad, India
2Department of Radiology and Imageology, Professor, Nizam’s Institute of Medical Sciences, Hyderabad, India
3Department of Radiology and Imageology, Assist Professor, Nizam’s Institute of Medical Sciences, Hyderabad, India
4Department of Radiology and Imageology, Head of Dept. and Professor, Nizam’s Institute of Medical Sciences, Hyderabad,India
Corresponding author: Dr. Sujata Patnaik, Department of Radiology and Imageology, Additional Professor,Nizam’s Institute of Medical Sciences, Hyderabad, Telangana State, India; Tel: +91 9490793534; E-mail: sujata_patnaik222@yahoo.co.in
Citation: Patnaik S, Jyotsnarani Y, Ramanjeneyulu HVK, Ramamurti S. Imaging of Osseous Lesions in Langerhans Cell Histiocytosis (LCH). Indian J Appl Radiol. 2017; 3(1): 114.
Copyright © 2017 Patnaik S. et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Applied Radiology | Volume: 3, Issue: 1
Submission: 24/07/2017; Accepted: 29/08/2017; Published: 11/09/2017
Abstract
Introduction: Langerhans Cell Histiocytosis (LCH) is a rare condition resulting from idiopathic proliferation of histiocytes and can affect any organ but is more often seen in bone, lung, skin, lymph nodes and endocrine glands. This paper is aimed at analyzing the imaging patterns of osseous involvement in cases of LCH.
Material and methods: It is a retrospective analysis of 18 histopathologically proven cases of LCH with osseous involvement done at our institute over the last 5 years.
Results: Of the total patients, 13 were males. Most were aged less than 10 years old. The bones involved were skull (n=9), long bones (n=6), vertebrae (n=5), pelvis (n=3), rib (n=1) and clavicle (n=1). Enhancement of soft tissue component was seen in 10 cases. Radiological features depend on site of involvement and phase of disease. Early phase lesions are lytic poorly defined. Lamellated periosteal reaction along with pathological fracture was noted in some. Later, the lesions became more clearly defined with sharp border. Chronic lesions were sclerotic. In our study, involvement of clavicle and posterior element of vertebrae and more affection of cervical than thoracic spine are unusual findings.
Conclusions: Though LCH is common in children less than 2 years, it can occur at any age. Skull involvement is the most common site for bony lesions. Unusual sites like clavicle may be involved. We observed that cervical spine is frequently affected and posterior element involvement is also not uncommon. Full skeletal survey with appropriate imaging is recommended after an initial diagnosis.
Keywords: Langerhans cell Histiocytosis; Eosinophilic granulomas; Hand schuler christian disease; Letterer disease
Introduction
Langerhans Cell Histiocytosis (LCH), previously referred as Histiocytosis X, is a clonal non-neoplastic disorder in which there is idiopathic proliferation of histiocytes resulting in focal or systemic manifestations. There can be painful swelling and sometimes pathological fracture can occur. Depending on its location and spread to adjacent tissues, the symptoms like proptosis, otitis media, hearing loss, spinal cord compression, loose tooth or Diabetes Insipidus (DI) can be the presenting feature [Figure 1]. It is a rare disorder with a reported Incidence of 2-5 cases per million per year in young adults <15 years and 1-2 cases per million per year in adults. It accounts for less than 5% of all primitive bone tumors [Figure 2]. It can affect any organ but is more often seen in bone, lung, skin, ln, ears, endocrine glands (except adrenal and gonads, pituitary gland, thymus), CNS, GIT, liver, spleen, bone marrow and blood [Figure 3].
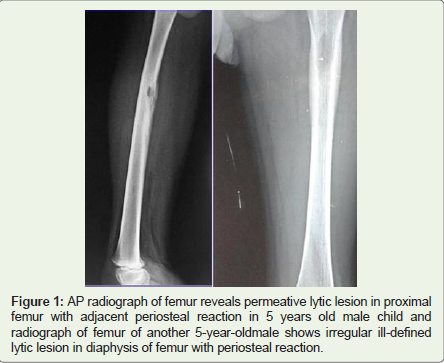
Figure 1: AP radiograph of femur reveals permeative lytic lesion in proximal femur with adjacent periosteal reaction in 5 years old male child and radiograph of femur of another 5-year-oldmale shows irregular ill-defined lytic lesion in diaphysis of femur with periosteal reaction.
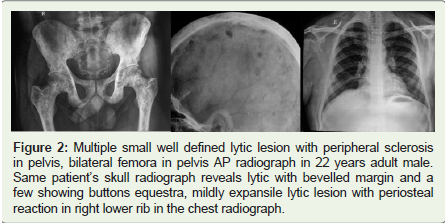
Figure 2: Multiple small well defined lytic lesion with peripheral sclerosis in pelvis, bilateral femora in pelvis AP radiograph in 22 years adult male. Same patient’s skull radiograph reveals lytic with bevelled margin and a few showing buttons equestra, mildly expansile lytic lesion with periosteal reaction in right lower rib in the chest radiograph.
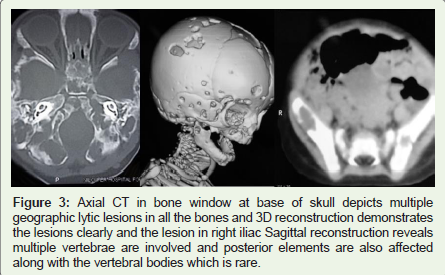
Figure 3: Axial CT in bone window at base of skull depicts multiple geographic lytic lesions in all the bones and 3D reconstruction demonstrates the lesions clearly and the lesion in right iliac Sagittal reconstruction reveals multiple vertebrae are involved and posterior elements are also affected along with the vertebral bodies which is rare.
Three variants-Eosinophilic Granuloma (EG), Hand Schuler Christian disease (HSC) and Letterer disease (LS) are described based on the pattern of presentation, but a distinction among these three entities is not always possible on clinic-radiological manifestations alone. EG often has bone involvement; single bone involvement is more common than poly-ostotic. In HSC multiple bones and multiple organs (skin, soft tissue, lymph node, liver, thymus and lung) are involved. A clinical triad - calvarial defect, exophthalmos and DI is a recognized pattern in HSC. LS Disease presents with multi organ involvement and is progressively fatal [Figure 4]. This paper is aimed at analysing the imaging patterns of osseous involvement in cases of Langerhans cell Histiocytosis, in view of its rarity.

Figure 4: AP skull radiograph of 2 years M child reveals multiple lytic lesions in bilateral frontal, temporal, parietal bones and contrast enhanced axial CT of another 2-year-oldchild shows lytic lesion with bevelled margin in bone window and contrast enhanced soft tissue in soft tissue window.
Material and Methods
It is a retrospective analysis of 18 histopathologically proven cases of LCH with osseous involvement done at our institute over the last 10 years. The database of the cases including the histopathologically and imaging reports were retrieved and analyzed.
Results
We analyzed 18 cases of histopathologically proven LCH. Of them 13 were males. Most of them (n=12) were aged less than 10 years old; 3 were in age range of 11 to 20 years and 3 were more than 20 years old. The site of occurrence and the bony lesions are depicted in the Table 1. The bones involved were skull (n=9), long bones (n=6), vertebrae (n=5), pelvis (n=3), rib (n=1) and clavicle (n=1). Enhancement of soft tissue component was seen in 10 cases.
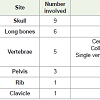
Table 1
Radiological Features
In children, the osseous involvement is seen in 75-90% of cases of LCH. Skull is the most common site affecting more than half. About 30% lesions occur in long bones. Other sites that are generally involved include vertebrae, pelvis, ribs and mandible. Hands and feet are uncommon sites of involvement. Multiple bone involvement in the same patients may be seen in 18-30% cases [5]. In study of 47 adults the jaw was the primary site in 30% followed by skull in 21% cases [6].
Radiological features depend on site of involvement and phase of disease. Early phase lesions are lytic poorly defined (Figure 1). Lamellated periosteal reaction may occur along with pathological fracture. Continuous periosteal reaction, cortical thickening are features of less aggressive lesion (Figure 1). Later, the lesions become more clearly defined with sharp border. Sometimes expanded appearance may be due to pre-existing soft tissue or due to lamellated peri-osteal reaction. Chronic lesions may resolve completely or may become sclerotic (Figure 2).
Skull
It is the skull that is most frequently involved and frontal bone is the commonest site. Skull was involved in 9 out of 18 (50%) of our cases. Parieto-temporal bone is the most common site in our observation (Figure 2). Skull lesions are lytic with endosteal scalloping cortical thinning. They are typically round or ovoid, measuring from 1 to 4 cms with well-defined non-sclerotic margin giving punched-out appearance (Figure 2). Uneven destruction of inner and outer table results in bevelled edge or double contour. Lytic lesion may contain a fragment called button sequestrum which refers to a piece of devitalized bone separated from surrounding bone (Figure 2). Button-sequestrum sign is specific for LCH. The number and size of skull lesions may increase with confluent areas resulting in geographic skull (Figure 3). Lesions may be associated with soft tissue which is isodensein T1 and hyper in T2 W images.
Homogenous enhancement is seen in CT and MRI (Figure 4). Sometimes adjacent dural enhancement may be observed on MRI. The differentials include epidermoid and dermoid for a single lesion and when multiple lesions are present, it has to be differentiated from metastatic neuroblastoma [7,8].
Mandible
Typical lesion can cause ‘floating teeth’ appearance when it has to be differentiated from periodontal disease, hyperparathyroidism, metastases, multiple myeloma, ameloblatoma, osteomyelitis, lymphoma, alveolar squamous cell carcinoma or Ewing’s sarcoma (Figure 5) [9].
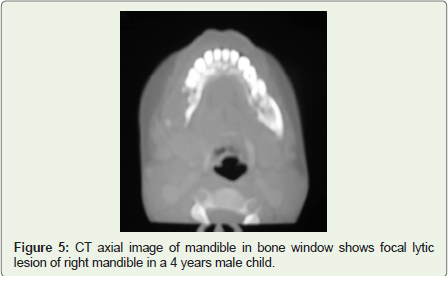
Figure 5: CT axial image of mandible in bone window shows focal lytic lesion of right mandible in a 4 years male child.
Flat bones
Rib involvement produces geographic moth-eaten or permeative pattern of lysis (Figure 2). It is sometimes associated with soft tissue involvement and may be associated with pathological fracture. Periosteal reaction is seen in pelvic bone lesion (Figure 4). Surrounding zone of sclerosis and well defined rim is seen in pelvic lesion, which is not seen in other flat bones. Scapular lesion appears as large irregular lytic area with little or no sclerosis. Expansile permeative lytic lesions occur in clavicle and when there is destruction of cortex, abundant periosteal reaction is observed (Figure 6). The common differentials may be considered are osteomyelitis and small round cell tumors [10].
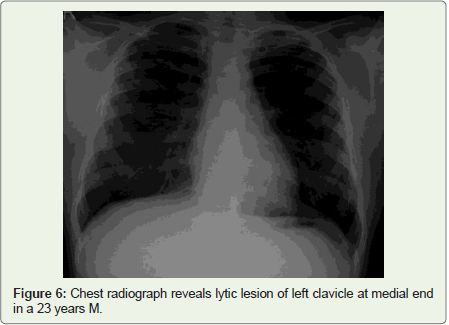
Figure 6: Chest radiograph reveals lytic lesion of left clavicle at medial end in a 23 years M.
Vertebra
LCH involvement of vertebra is known to occur in 10-18% of pediatric spinal tumor [11]. Thoracic vertebraeare more commonly involved (54%) than lumbar (35%), which is more than cervical vertebra (11%) (Figure 7) [12]. In contrast, majority of our cases have cervical (n=4) followed by dorsal (n=3) followed by lumbar vertebra (n=2). Solitary vertebra involvement occurs in 10% cases. Vertebral involvement was single level in 1 case and multiple in 4 of our series (Figure 7). Vertebral body is more involved and posterior elements are rare [13]. Involvement of posterior elements was observed in 3 of our 5 cases of spinal involvement which is unusual (Figures 7,8).

Figure 7: Lateral radiograph and T2W sagittal MRI images reveal collapse of D8, D11 vertebrae, axial T1W MRI reveals soft tissue, epidural component and involvement of posterior elements.
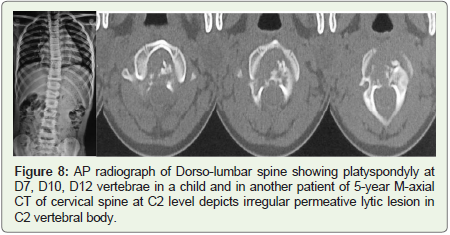
Figure 8: AP radiograph of Dorso-lumbar spine showing platyspondyly at D7, D10, D12 vertebrae in a child and in another patient of 5-year M-axial CT of cervical spine at C2 level depicts irregular permeative lytic lesion in C2 vertebral body.
The initial lesion may be lytic. Typically solitary, well defined withscalloped vertebral body. Alternatively the body of vertebra may be abnormally flattened. The intervertebral disc a little widened or is normal. Gradually vertebral collapse gives vertebra plana or ‘coin on edge’ appearance. Typical vertebral plana is reported in only 40% of LCH (Figure 8). It is more common in children [14,15].
Cervical lesion usually involves core of vertebral body with lytic lesion while in thoracic and lumbar area, there is more tendency for collapse. The collapse may be symmetrical or asymmetrical. Vertebra plana with sclerosis, coarsening of trabecular pattern and ‘bone within bone’ appearance of intra body osseous lesion are common features. Soft tissue component may be seen (Figure 7). Disc spaces are preserved. Vertebral height may be restored spontaneously or after treatment. Sometimes affected vertebra reverts to an almost normal configuration [16].
Long bones
Long bone involvement is seen in 30% cases, like our series showing 6 out of 18 (30%). In long bones femur is the most common site as in the present series (n=4) followed by tibia and humerus (Figure 1). Diaphysis is the most common site of long bone involvement. A welldefined lytic lesion with or without sclerotic margins is the classical appearance. Metaphysis can also be affected and rarely may extend to growth plate to involve epiphysis. Pure epiphyseal lesions are rare. Endosteal scalloping, cortical thinning, intra cortical tunneling, widening of medullary cavity are the most frequent changes that are noted (Figure 9). Sometimes lesion may be permeative and mimics malignancy. Sometimes lesion penetrates the cortex and extends to adjacent soft tissue (Figure 10). The endosteal scalloping appears as budding appearance in CT and MRI (Figure 10). Periosteal reaction may be aggressive or may be absent. Periosteal reactions may occur with or without pathological fracture. It may be thin, intermediate or more solid form and may be circumferential (Figure 1). At this stage it has to be differentiated from osteomyelitis, Ewing’s sarcoma or lymphoma (Figure 9). Sclerosis is noted with treatment with more defined margin and lesion may even disappear. Sometimes lesions may be mixed lytic and sclerotic due to chronicity with elements of healing [8].

Figure 9: 8-year-old female presented with a lesion in meta-diaphysis with intracortical tunneling of upper end of ulna in AP radiograph and permeative expansile lytic lesion with periosteal reaction in upper metaphysis of femur mimicking round cell tumor in another female child confirmed to be LCH on HPE.
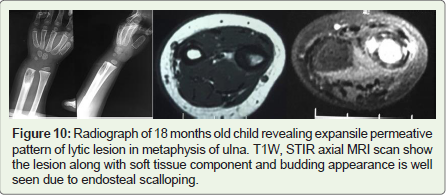
Figure 10: Radiograph of 18 months old child revealing expansile permeative pattern of lytic lesion in metaphysis of ulna. T1W, STIR axial MRI scan show the lesion along with soft tissue component and budding appearance is well seen due to endosteal scalloping.
Unusual Skeletal Changes
Unusual sites are epiphysis, trans-physeal plate extension, button sequestra in extra cranial sites, dural extension of vertebral lesion, involvement of clavicle, posterior arch, small bones of hands and feet [Figure 17]. In our study, involvement of clavicle and posterior element of vertebrae, more affection of cervical spine than thoracic spine and extra-skeletal affection are unusual findings.
Poor Prognostic Factors
Presentation before two years, poly-ostotic (>3bones), bone lesion spreading to adjacent soft tissue, hepato-splenomegaly and bone marrow involvement are considered as poor prognostic signs [18].
Role of Imaging Work Up
Most of bony lesions are detected by radiographs and had been used conventionally for several years. Radionuclide bone scan typically shows ‘hot’ spot and nuclear scan may reveal additional lesions in complex sites. CT and MRI are done for better delineation of the lesions. CT is particularly helpful in confirming periosteal reactions and cortical erosion. It facilitates the evaluation of skeletal areas difficult to assess by radiographs such as skull, facial bones and pelvic bones. MRI is most suited for assessment of involvement of paravertebral soft tissue. PET-CT is for localization of multiplicity of lesions and for treatment response. The activity of lesions can be assessed by MRI or PET scanning [19].
Treatment
EG may resolve spontaneously and resolution is unaffected by mode of therapy. Surgery, Radiation, Chemotherapy, steroids either alone or in combination are tried. Surgery is indicated when neurologic affection is found.
Conclusion
Though LCH is common in children less than 2 years, it can occur at any age. Skull involvement is the most common site for bony lesions. Unusual sites like clavicle may be involved as seen in one of our cases. Though it is described in literature that thoracic spine is affected more commonly, we observed that cervical spine is frequently affected and posterior element involvement is also not uncommon. Enhancing soft tissue is also commonly observed. After initial diagnosis in a case of LCH, it is crucial to find out if there is a single or multiple lesions for which full skeletal survey with appropriate imaging is recommended.
References
- Yu RC, Chu C, Buluwela L, Chu AC (1994) Clonal proliferation of langerhans cells in langerhans cell histiocytosis. Lancet 343: 767-768.
- Madrigal-Martínez-Pereda C, Guerrero-Rodríguez V, Guisado-Moya B, Meniz-García C (2009) Langerhans cell histiocytosis: Literature review and descriptive analysis of oral manifestations. Med Oral Patol Oral Cir Bucal 14: E222- E228.
- Hoover KB, Rosenthal DI, Mankin H (2007) Langerhans cell histiocytosis. Skeletal Radiol 36: 95-104.
- Karagoz Guzey F, Bas NS, Emel E, Alatas I, Kebudi R (2003) Polyostotic monosystemic calvarial and spinal langerhans cell histiocytosis treated by surgery and chemotherapy. Pediatr Neurosurg 38: 206-211.
- Stull MA, Kransdorf MJ, Devaney KO (1992) Langerhans cell histiocytosis of bone. Radiographics. 12: 801-823.
- Baumgartner I, von Hochstetter A, Baumert B, Luetolf U, Follath F (1997) Langerhans'-cell histiocytosis in adults. Med Pediatr Oncol 28: 9-14.
- Cochrane LA, Prince M, Clarke K (2003) Langerhans' cell histiocytosis in the pediatric population: Presentation and treatment of head and neck manifestations. J Otolaryngol 32: 33-37.
- Meyer JS, De Camargo B (1998) The role of radiology in the diagnosis and follow-up of langerhans cell histiocytosis. Hematol Oncol Clin North Am 12: 307.
- Avril L, Lombardi T, Ailianou A, Burkhardt K, Varoquaux A, et al. (2014) Radiolucent lesions of the mandible: A pattern-based approach to diagnosis. Insights Imaging 5: 85-101.
- Wilner D (1982) Radiology of bone tumors and allied disorders. Saunders pp. 4258.
- Copley L, Dormans JP (1996) Benign pediatric bone tumor. Evaluation and treatment. Pediatr Clin North Am 43: 949-966.
- Sanchez RL, Llovet J, Moreno A, Galito E (1984) Symptomatic eosinophilic granuloma of spine: Report of two cases and review of the literature. Orthopedics 7: 1721-1726.
- Maggi G, de Sanctis N, Aliberti F, Rega AN (1996) Eosinophilic granuloma of C4 causing spinal cord compression. Child’s Nerv Syst 12: 630-632.
- Bertram C, Madert J, Eggers C (2002) Eosinophilic granuloma of the cervical spine. Spine (Phila PA 1976) 27: 1408-1413.
- Garg S, Mehta S, Dormans JP (2004) Langerhans cell histiocytosis of the spine in children: Long-term follow-up. J Bone Joint Surg Am 86: 1740-1750.
- Jiang L, Guang Liu X, Zhong WQ, Jun Ma Q, Wei F, et al. Langerhans cell histiocytosis with multiple spinal involvement. Eur Spine J 20: 1961-1969.
- Hindman BW, Thomas RD, Young LW, Yu L (1998) Langerhans cell histiocytosis: Unusual skeletal manifestations observed in thirty-four cases. Skeletal Radiol 27: 177-181.
- Kilpatrick SE, Wenger DE, Gilchrist GS, Shives TC, Wollan PC, et al. (1995) Langerhans' cell histiocytosis (Histiocytosis X) of bone. A clinicopathologic analysis of 263 pediatric and adult cases. Cancer 76: 2471-2484.
- Binkovitz LA, Olshefski RS, Adler BH (2003) Coincidence FDG-PET in the evaluation of langerhans' cell histiocytosis: Preliminary findings. Pediatr Radiol 33: 598-602.