Case Report
Neurocutaneous Melanosis: A Rare Case
Karnavat Chandresh O1*, Mehta Rajeev U2, Shah Arun B3 and Khartode Chhagan P4
1Senior Resident, Department of Radiology, Saifee Hospital, Mumbai, India
2Chairman, Department of Radiology, Saifee Hospital, Mumbai, India
3Consultant, Department of Neurology, Saifee Hospital, Mumbai, India
4Senior resident, Department of Internal Medicine, Saifee Hospital, Mumbai, India
Corresponding author: Chandresh O. Karnavat, Department of Radiology, Saifee Hospital, Mumbai, India, Tel:+919833541813; E-mail: chand.k.13@gmail.com
Citation: Karnavat CO, Mehta RU, Shah AB, Khartode CP. Neurocutaneous Melanosis: A Rare Case. Indian J Appl Radiol. 2017;3(1): 113.
Copyright © 2017 Karnavat CO. et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Applied Radiology | Volume: 3, Issue: 1
Submission: 26/01/2017; Accepted: 03/04/2017; Published: 07/04/2017
Abstract
We report a 15-year-old male patient who presented with sudden onset generalized tonic clonic convulsions and had multiple extensive large pigmented nevi covering entire back. Head CT revealed hyperdense foci in bilateral temporal lobes. MR imaging of the brain revealed multiple T1-Weighted Imaging (T1W) hyperintense foci in bilateral anterior temporal lobes with leptomeningeal enhancement. These findings along with skin lesions are suggestive of neurocutaneous melanosis.
Abbreviations: T1W: T1-Weighted Imaging; SWI: Susceptibility-Weighted Imaging; T2W: T2-Weighted; DWI: Diffusion-Weighted Imaging; FLAIR: Fluid Attenuated Inversion Recovery Abbreviations: T1W: T1-Weighted Imaging; SWI: Susceptibility-Weighted Imaging; T2W: T2-Weighted; DWI: Diffusion-Weighted Imaging; FLAIR: Fluid Attenuated Inversion Recovery
Case Report
15-year-old male patient was brought to the casualty department with a first episode of sudden onset generalized tonic clonicconvulsions followed by a fall. There was no history of any other neurological symptoms till date. General examination revealed multiple extensive large pigmented nevi covering entire back (>3) (Figure 1), which were present since birth without any change in size.Family history was non-contributory. CSF revealed normal glucose (63 mg/dl) and protein (460 mg/L) levels with a white cell count of 2 cells/mm3. The CSF findings were thus unremarkable.

Figure 1: Multiple extensive hairy pigmented nevi seen over the back.
Head CT scan revealed small focal hyperdense areas in bilateral temporal lobes (60.5 Hounsfield Unit) (Figure 2) simulating hemorrhagic contusions. MR imaging of the brain revealed multiple T1W hyperintense foci in bilateral anterior temporal lobes corresponding to hyperdense areas noted in CT scan (Figure 3). In addition, a hyperintense lesion was also seen in right frontal lobe (Figure 4). These lesions were persistently hyperintense on T1W fat saturated (sat) images. These areas were not appreciated on T2-Weighted (T2W) images. No evidence of blooming on Susceptibility-Weighted Imaging (SWI) images was noted thus ruling out hemorrhage. No area of restricted diffusion was noted on Diffusion-Weighted Imaging (DWI) images. No perifocal vasogenic edema was seen. Extensive leptomeningeal enhancement was seen on post-contrast Fluid Attenuated Inversion Recovery (FLAIR) images (Figure 5). MR imaging of spine was unremarkable.

Figure 2: Axial Plain CT reveals hyperdense areas in bilateral anterior temporal lobes.

Figure 3: Plain axial T1W images show multiple focal hyperintense lesions seen in bilateral temporal lobes.
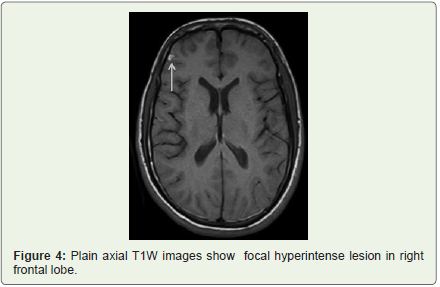
Figure 4: Plain axial T1W images show focal hyperintense lesion in right frontal lobe.
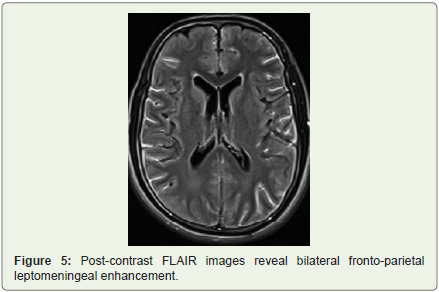
Figure 5: Post-contrast FLAIR images reveal bilateral fronto-parietal leptomeningeal enhancement.
Giant congenital melanotic nevi in the trunk along with classical locations of intraparenchymal melanosis and leptomeningeal melanosis were thus suggestive of neurocutaneous melanosis. The patient was discharged on anti-convulsants with regular follow up.
Discussion
Neurocutaneous melanosis is a rare phakomatosis resulting from congenital dysplasia of the neuroectodermal melanocyte precursor cells [1]. The prevalence of large congenital melanotic nevi in skin is estimated to occur in less than one in 20,000 newborns [2]. The risk of neurocutaneous melanosis in these patients varies from 1 to 12% [2]. Though disease is considered sporadic, Kinsler et al. have reported post-zygotic mutations in codon 61 of NRAS gene to be the cause of this disorder [1,3]. This disease usually presents at 2 years of life, however, a second smaller peak of symptom development occurs during puberty or the young adult years as in our case [4]. Clinical manifestations include focal or generalized seizures, aphasia, and motor or cranial nerve deficits [4].
Though CT is not optimal compared with MR imaging for demonstrating neurocutaneous melanosis, the foci of melanin containing cells may appear as areas of high attenuation. Rebecca YT Ng et al. have reported a case of diffuse leptomeningeal melanocytosis showing the areas of cisternal hyperdensity mimicking subarachnoid hemorrhage; similar to our case in which intraparenchymal melanosis mimics hemorrhagic contusions on CT scan [5]. MR imaging findings of neurocutaneous melanosis include foci (typically 3 cm or less in size) of T1 and T2 shortening within the brain parenchyma and meninges [1]. These imaging characteristics of melanin are thought to be caused by the presence of paramagnetic free radicals (indolesemiquinones and semiquinones) [1]. Most common location of these foci is in the anterior temporal lobe (especially in the region of the amygdala) followed by cerebellar white matter, cerebellar nuclei, and the brainstem [1]. Melanin appears isointense to hypointense on T2W images [6]. Leptomeningeal enhancement has been reported in neurocutaneous melanosis [1].
Substances that appear hyperintense on T1 include methemoglobin, melanin, lipid, protein, and minerals. Findings of absence of blooming on SWI and the persistence of hyperintensity on T1W fat sat images along with the classical location of intraparenchymal lesions and leptomeningeal enhancement in our case is suggestive of melanotic lesions in the brain.
Another differential diagnosis of melanin containing lesion in the brain in a patient with skin lesions includes metastatic malignant melanoma. However multiple foci of metastatic melanoma are predominantly located at the gray-white matter junction and have surrounding vasogenic edema (similar to other metastasis) with postcontrast enhancement [1].
Follow up is suggested to watch for malignant degeneration into melanoma in the brain by MRI (indicated by progressive growth, surrounding vasogenic edema or mass effect, or development of central necrosis) and in skin by clinical examination (changes in color, size, shape, rapid growth rate, proliferative nodules or ulceration) warranting the need of biopsy.
The treatment is palliative and treatment options include systemicintrathecal chemotherapy, radiotherapy and ventriculoperitoneal shunt in cases of hydrocephaly [4,6]. Regardless of the treatment, the prognosis is bad [6].
Conclusion
Thorough clinical examination and appropriate neuroimaging will help to identify this rare and dreadful phakomatosis.
References
- Smith AB, Rushing EJ, Smirniotopoulos JG (2009) Pigmented lesions of the central nervous system: radiologic-pathologic correlation. Radiographics 29: 1503-1529.
- Scattolin MA, Lin J, Peruchi MM, Rocha AJ, Masruha MR, et al. (2011) Neurocutaneous melanosis: follow-up and literature review. J Neuroradiol 38: 313-318.
- Kinsler VA, Thomas AC, Ishida M, Bulstrode NW, Loughlin S, et al. (2013) Multiple congenital melanocytic nevi and neurocutaneous melanosis are caused by postzygotic mutations in codon 61 of NRAS. J Invest Dermatol 133: 2229-2236.
- Acosta FL, Binder DK, Barkovich AJ, Frieden IJ, Gupta N (2005) Neurocutaneous melanosis presenting with hydrocephalus. Case report and review of the literature. J Neurosurg 102(1 Suppl): 96-100.
- Rebecca YT, Deyond Siu YW, Wong GK, HK Ng, Poon WS (2013) An uncommon mimic of spontaneous subarachnoid haemorrhage. Hong Kong Med J 19: 80-81.
- Flores-Sarnat L (2013) Neurocutaneous melanocytosis. Handb Clin Neurol 111: 369-388.