Research Article
Comparison between Ultrasonography andConventional Radiography in the Detection of Bony Fractures
Seema Sharma1*, Poonam Ohri1, Harjinder Singh2 and Sohan Singh1
1Department of Radiodiagnosis, Government Medical College, Basant Nagar, Majitha Road, Amritsar, Punjab, India
2Department of Pediatrics, Government Medical College, Basant Nagar, Majitha Road, Amritsar, Punjab, India
Corresponding author:Seema Sharma, Department of Radiodiagnosis, Government Medical College, 17-A,Basant Nagar, Majitha Road, Amritsar, Punjab, India, Tel: 08146860055; E-mail: drgdsharda@gmail.com
Citation: Sharma S, Ohri P, Singh H, Singh S. Comparison between Ultrasonography and Conventional Radiography in the Detection of Bony Fractures. 02 Indian J Appl Radiol. 2017;3(1): 112.
Copyright © 2017 Sharma S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Applied Radiology | Volume: 3, Issue: 1
Submission: 09/09/2016; Accepted: 17/02/2017; Published: 22/02/2017
Abstract
Aims: To evaluate the efficacy of ultrasound in diagnosing the presence or absence of fractures in clinically suspected patients in comparison with the conventional radiography.
Settings and design: Fifty patients of any age group and either sex coming to emergency wing or orthopaedic outdoor or indoor and other departments at our institution with clinically suspected fractures were included in the study.
Materials and methods:The patients were examined with conventional radiograph (CR) followed by ultrasonography done using real-time scanner with a high frequency linear transducer in both longitudinal and transverse planes. The results of radiography and ultrasonography were compared to see their relative efficacy in the detection of fractures.
Results: The study showed that the sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and accuracy of the CR against USG are 100% each in the case of long bone fracture detection. However, in the case of flat bone sensitivity, specificity, PPV, NPV and accuracy of the CR against USG was 50%, 100%, 100%, 33.3% and 60%, respectively. Further, in the case of short bone fracture detection, sensitivity, specificity, PPV, NPV and accuracy of the CR against USG are 60%, 100%, 100%, 33.3% and 66.67%, respectively. So the overall sensitivity, specificity, PPV, NPV andaccuracy of CR against USG in this present study came out to be 82.35%, 100%, 100%, 72.73% and 88%, respectively.
Conclusions: USG is a cost effective, easily available, portable and radiation free imaging technique for the detection of the superficially situated fractures. It is found superior to the CR in the detection of the fractures of the flat and short bones and equally sensitive in the long bone fractures.
Keywords: CR; USG; Fractures; RTA; Scaphoid; Bone; Assault
Introduction
Injury is a major cause of death and disability worldwide [1]. Bone fractures are common injuries among them. Bone fracture is a surgical condition in which there is a break in the continuity of the bone. They occur when a sizable force causes the bone to break. Falls, moving collisions and forceful blows are traumatic causes of bone fractures. Diseases that weaken the bones and overuse can also lead to pathological bone fractures [2].
There are four major types of bones on the basis of shape-long,short, flat, sesamoid and irregular [3].
All fractures were initially detected on radiograph [4]. However, the fractures may at times be imperceptible on conventional radiographs, either because they are subtle or occult, obscured by overlapping structures, or non-perpendicular to the X-ray beam. A fracture may also involve cartilage and be undetectable, especially in skeletally immature children. Therefore, complimentary imaging would be desirable to eliminate or confirm the presence of a fracture to avoid short-term and long-term complications [5,6].
Among carpal fractures, scaphoid fractures are by far the most frequently observed and may lead to long-lasting sequelae. However, immediately after injury, up to 65% of scaphoid fractures remain radiographically occult. Thus, in patients with suspected scaphoid fractures (i.e. occult scaphoid fractures), the wrist has to be placed in a scaphoid cast for at least 10 days, until the scaphoid fracture is ruled out with follow-up radiographs. This strategy, however, means that some patients without a fracture would have their wrist immobilized for several days, which is inappropriate and results in both a reduction in the quality of life and an increase in health care costs [7]. Because of its excellent sensitivity (95-100%) and specificity(100%), Magnetic Resonance (MR) imaging has been advocated as the imaging modality of choice in these patients; however it is not widely available in developing countries and is costly.
High-spatial-resolution Ultrasonography (USG), however, may be an alternative imaging modality in patients with occult scaphoid fractures. Technical improvements in sonography have led to higher spatial resolution of this diagnostic tool, and, thus, high-spatialresolutionUS may depict subtle post-traumatic changes of the cortex and/or periosteum, which may already be present immediately after the injury but which are not depicted on conventional radiographs. Furthermore, high-spatial-resolution US, compared with MR imaging, is more readily accessible, less time-consuming, and considerably less expensive [7].
The most frequently seen injury in patients admitted to outpatient clinics and emergency departments with blunt thoracic trauma is ribfractures. Non-displaced rib fractures may be frequently missed with using only direct radiography for diagnosis. Many studies have shown an increased sensitivity of Ultrasonography (USG) in rib fractures in the literature [8].
USG has shown excellent results in the detection of the diaphyseal,nasal, facial and sternal fractures [9-12].
As bone is a natural obstacle to the transmission of sound at high frequency, so there is a large difference in acoustic impedance between the soft tissue and bone, resulting in a strong reflection from the bone. Hence, USG presents an ideal situation for imaging the bony contour. Any imperfections (e.g. steps, breaks, periosteal reactions) should therefore be easily visible [10].
The ultrasongraphic features of fractures comprise
Cortical disruption, Cortical irregularity, Reverberation, Posterior acoustic shadowing, Periosteal elevation and Hematoma. However, the hallmark of an acute fracture is a discontinuity of the bone cortex with a possible step off deformity [6].
Subjects and methods
Fifty patients of any age group and either sex coming to emergency wing or orthopaedic outdoor or indoor and other departments at ourinstitution with clinically suspected fractures were included for the study.
Exclusion criteria
Open, unstable or suspected compound fractures, unstable patients with deranged vitals and pregnant females. Each patient was subjected to detailed history, local examination, and conventional radiography with appropriate views. This was followed by ultrasonography using real time scanner (Philips Envisor C and Esaote) with a high frequency linear transducer in both longitudinal and transverse planes. The results of radiography and ultrasonography were compared to see their relative efficacy in the detection of fractures.
Examination technique
Ultrasound was done using a real time scanner (Philips Envisor C and Esaote) with a 5-12 MHz Broad Band linear array probe with musculoskeletal preset. Suspected site was examined patiently in both transverse and longitudinal planes. Care was taken to scan very lightly over the site. On USG, breech in the continuity of the cortex of the bone was used as the criterion to suggest a fracture as it is the most definitive and reliable factor in diagnosing a fracture on ultrasonography. A clear disruption of cortical bone as small as 1-2 mm was detected. Displacement of the fractured ends was also appreciated with the USG probe as step off deformity or avulsion of a bony segment. Limit of about 2 mm was taken as a criterion for deciding displacement to be present or absent.
Results
In the present study of 50 cases, the majority of the cases 43(86%) were in the age group of 21-60 years, of which 22 (44%) were between 21 and 40 years and 21 cases (42%) were between 41 and 60 years. Five (10%) patients were < 20 years of age group, while 2 (4%) were > 60 years. The youngest patient included in the study was a one year old male child and the oldest patient was a male of 65 years of age. Most of the patients were males 42 (84%) and the number of female patients were 8 (16%). Out of the 50 cases, 23 (46%) cases had a history of fall, 15 (30%) cases had history of road traffic accident and the rest 12 (24%) had a history of alleged assault.
In majority of the cases, radiographic projections required weretwo in 37 (74%) subjects. Maximum projections done were four in 7 (14%) cases and minimum one in 4 (8%) cases. In rest 2 (4%) cases 3 projections were done. In our study, a long bone was injured in 34 (68%) cases, flat bone in 10 (20%) cases and short bone in the rest 6 (12%) subjects. Conventional radiography with appropriate projections detected fractures in 28 (56%) subjects and did not reveal the fracture in rest 22 (44%) subjects. However, USG detected fractures in 34 (68%) cases and was negative in 16 cases.
Our study showed that both conventional radiography andultrasonograhy detected fractures in 21 (61.76%) cases involvinglong bones and both modalities ruled out bony fractures in 13(38.24%) cases (Table 1). In case of flat bone fractures, conventionalradiography detected fractures in 4 (40%) cases and was negative inrest 6 (60%) cases, whereas USG detected fractures in 8 (80%) casesand was negative in 2 (20%) cases (Table 1).
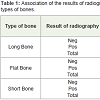
Table 1: Association of the results of radiography with result of USG in different types of bones.
In case of short bone fractures, CR picked up fractures in 3(50%) subjects and was negative in rest 3 (50%) subjects but USG was positive in 5 (83.55%) cases and confirmed no fracture in one (16.45%) (Table 1).
The present study showed that sensitivity, specificity, PositivePredictive Value (PPV), Negative Predictive Value (NPV) and accuracy values of the CR against USG were 100% in the case of long bone fracture detection. However, in the case of flat bone, sensitivity, specificity, PPV, NPV and accuracy values of the CR against USG were 50%, 100%, 100%, 33.3% and 60%, respectively. Further, in the case of short bone fracture detection, sensitivity, specificity, PPV, NPV and accuracy values of the CR against USG were 60%, 100%, 100%, 33.3% and 66.67%, respectively (Table 2). So overall sensitivity, specificity, PPV, NPV and accuracy values of CR against USG in this present study came out to be 82.35%, 100%, 100%, 72.73% and 88%, respectively (Table 3).
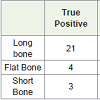
Table 2: Sensitivity, Specificity, PPV, NPV and Accuracy of radiography against USG in different types of bones.
Table 3: Overall Sensitivity, Specificity, PPV, NPV and Accuracy of radiography against USG.
Discussion
The injuries have been traditionally evaluated by clinicalexamination and radiographic imaging. But radiographs may be contraindicated in certain situations such as in pregnant women [11].
The high number of negative conventional radiography results is likely due to inappropriate indication for bone X-ray as well as due to the low sensitivity of this modality for certain types of fractures. It leads to unwanted exposure of the patients to harmful ionizing radiations, missed diagnosis and in appropriate treatment as well financial burden [9]. This indicates the need for alternative methods for accurate detection of fractures, without risk of radiation exposure. Ultrasound may fill this role [9]. Ultrasound shows promise as a diagnostic tool in detection of fractures. The development of handheld ultrasound systems may therefore enable a means of more quickly identifying clinically significant fractures, through more rapid image acquisition and simultaneous interpretation at the bed side. Because of their small size these are useful in locations where traditional radiography and experienced physicians are not available [9].
Long bones
Both conventional radiography and ultrasonography detectedfractures in 21 cases of long bones and both ruled out them in 13 casessuggesting that in cases of long bone both the modalities showed equalsensitivity, specificity, NPV, PPV and accuracy (Figure 1). A study done in 2004 found that the USG had high sensitivity and specificity for long bone fracture detection versus traditional radiography and CT [12]. In a study done in 2012 on emergency USG in the detection of pediatric long bone fractures showed 100% sensitivity for the diaphyseal fractures [13]. A study suggested that USG may gain a more prominent role in pregnant and pediatric population as well as in mass casualty scenarios [14,15].
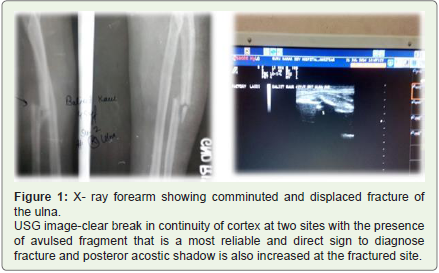
Figure 1: X- ray forearm showing comminuted and displaced fracture of the ulna.USG image-clear break in continuity of cortex at two sites with the presence of avulsed fragment that is a most reliable and direct sign to diagnose fracture and posteror acostic shadow is also increased at the fractured site.
Flat bones
In the present study, we had three patients of suspected nasal bone injury. Out of these one case was positive and two cases were negative on CR. While on USG, two cases were positive, and one case was negative for fracture. Complexity of the facial bones and the density of the cranial base make the conventional radiography inadequate for fractures of the facial bones. The low-accuracy rate is usually associated with nasal bone radiographs due to high percentage of false-negative and false-positive results (Figure 2). A study done in 2011 showed the ultrasonographical diagnosis of nasal bone fractures yielded 100% accuracy, sensitivity, specificity, NPV and PPV [6].

Figure 2: X-ray nasal bones-unremarkable USG image shows breech in the continuity of the left nasal bone.
We enrolled 4 patients with chest trauma with the suspicion of rib fracture. Mode of injury was RTA. Two cases were detected positive on both the modalities and one case was proved negative on both investigations. But in one case chest X-ray was negative, however, USG picked up breech in the cortex at the site of the maximum tenderness which was confirmed on CT scan. Along with the detection of the breech in the cortex, limited pleural effusion was also seen in one case of rib fracture with USG. Pleural effusion was an additional finding which further motivated to look for the occult fracture. Moreover, chondral rib fractures are almost invisible on chest x ray unless the fracture involves a strongly calcified cartilage. A study done in 1999 showed that sonography detected ten times more fractures than radiography (Figure 3). Sensitivity, specificity, NPV, and PPV of CR were 15%, 100%, 20%, 100% in detecting rib fracture and 90%, 100%, 69%, and 100% with USG respectively [16]. In the present study, high resolution ultrasonography was able to pick up the discontinuity of the cortex of the frontal bone in two cases for which radiography was negative [17]. This study demonstrated CR to be less sensitive and having lower negative predictive value as compared to USG in depicting cortical discontinuity in fractured small bones. A study conducted in 2005 concluded that the global sensitivity of high resolution sonography for detection of the occult scaphoid fractures was 100% and specificity 79% [15] (Figure 4). This study had certai limitations that included small size of sample and relative lack of fractures at sites near joints (ankles, knees, elbows) [18-21].
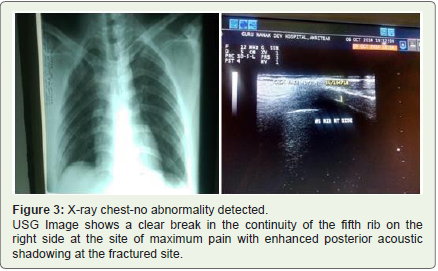
Figure 3: X-ray chest-no abnormality detected. USG Image shows a clear break in the continuity of the fifth rib on the right side at the site of maximum pain with enhanced posterior acoustic shadowing at the fractured site.

Figure 4: X-ray four views for scaphoid bone-unremarkable USG image shows the fracture of the scaphoid bone with minimal periosteal reaction.
Conclusion
Ultrasonographic examination might act as a substitute forradiography in detection of bony fractures, thus saving the patient from radiation exposure. Further research should be directed at studying the routine use of the ultrasound in the detection of fractures.
References
- Weinberg ER, Tunik MG, Tsung JW (2010) Accuracy of clinician-performed point-of-care ultrasound for the diagnosis of fractures in children and young adults. Injury 41: 862-868.
- Maheshwari J (2005) Orthopedic trauma. In: Essential orthopedics. 3rded, New Delhi, Mehta Publishers, pp. 330.
- Balaban NE, Bobick J (2008) Skeletal system. In: The handy anatomy answer book. Visible Ink Press Publishers, pp. 376.
- Zebouni SH, Khalil SA, Roukos S, Moussa ML, Smayra T, et al. (2008) Musculoskeletal imaging limb fractures: ultrasound imaging features. J Radiol 89: 557-563.
- Platon A, Poletti PA, Van Aaken J, Fusetti C, Della Santa D, et al. (2011) Occult fractures of scaphoid:the role of ultrasonography in the emergency department. Skeletal Radiol 40: 869-875.
- AL-Bahrany ZM, AL-Nakib LH (2011) Comparison between high-resolution ultrasonography and conventional radiography in the diagnosis of nasal bone fractures. Tikrit Journal of Dental Sciences 1: 6-13.
- Herneth AM, Siegmeth A, Bader TR, Ba-Ssalamah A, Lechner G, et al. (2001) scaphoid fractures: evaluation with high-spatial-resolution us-initial results. Radiology 220: 231-235.
- Uzun M, Beksac B, Karatas A, Kucukdurmaz F, Kircali BA, et al. (2013) Ultrasonography as a better diagnostic efficiency in rib fracture. J Exp Clin Med 30: 133-135.
- Thiede O, Krömer JH, Rudack C, Stoll W, (2005) Comparison of ultrasonography and conventional radiography in the diagnosis of nasal fractures. Arch Otolaryngol Head Neck Surg 131: 434-439.
- Nickson C, Rippey J (2011) Ultrasonography of sternal fractures. Australas J Ultrasound Med 14: 6.
- Waterbook AL, Adhikari S, Stolz U, Adrion C (2013) The accuracy of point-of-care ultrasound to diagnose long bone fractures in the ED. Am J Emerg Med 31: 1352-1356.
- Singh KS, Jayachandran S (2014) A comparative study on the diagnostic utility of ultrasonography with conventional radiography and computed tomography scan in detection of zygomatic arch and mandibular fractures. Contemp Clin Dent 5: 166-169.
- Barata I, Spencer R, Suppiah A, Raio C, Ward MF, et al. (2012) Emergency ultrasound in the detection of pediatric long-bone fractures. Pediatr Emerg Care 28: 1154-1157.
- Patel DD, Blumberg SM, Crain EF (2009) The utility of bedside ultrasonography in identifying fractures and guiding fracture reduction in children. Pediatr Emerg Care 25: 221-225.
- Fusetti C, Poletti PA, Pradel PH, Garavaglia G, Platon A, et al. (2005) Diagnosis of occult scaphoid fracture with high-spatial-resolution sonography: a prospective blind study. J Trauma 59: 677-681.
- Griffith JF, Ranier TH, Ching AS, Law KL, Cocks RA, et al. (1999) Sonography compared with radiography in revealing acute rib fracture. AJR Am J Roentgenol 173: 1603-1609.
- Parri N, Crosby BJ, Glass C, Mannelli F, Sforzi I, et al. (2013) Ability of emergency ultrasonography to detect pediatric skull fractures: a prospective, observational study. J Emerg Med 44: 135-141.
- Hubner U, Schlicht W, Outzen S, Barthel M, Halsband H (2000) Ultrasound in the diagnosis of fractures in children. J Bone Joint Surg [Br] 82: B1170-B1173.
- McKinnis LN (2014) Fundamentals of musculoskeletal imaging. 4th Ed F.A. Davis Company pp. 752.
- Tayal VS, Antoniazzi J, Pariyadath M, Norton HJ (2007) Prospective use of ultrasound imaging to detect bony hand injuries in adults. J Ultrasound Med 26: 1143-1148.
- Marshburn TH, Legome E, Sargsyan A, Shannon Melton James Li, Vicki A. Noble, et al. (2004) Goal-directed ultrasound in the detection of long-bone fractures. J Trauma 57: 329-332.