Case Report
Rare Artery of Percheron Infarct -Clinico- Radiological Diagnosis
Rashmeet Kaur*, Niharika Mahajan, Sandeep Bansal
Corresponding author: Rashmeet Kaur, Department of Radiology (Gian Sagar Medical College, Banur, Punjab), India, Mob No- 09417060705; E-mail: dr.rashmeet@gmail.com
Citation: Rashmeet K, Niharika M, Sandeep B. Dyke-Davidoff-Masson Syndrome/ Cerebral Hemiatrophy in an Adult Male : A Rare Imaging Case. Indian 02 J Appl Radiol. 2015;2(1): 108.
Copyright © 2015 Tejas Mohan Tamhane SG. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Applied Radiology | Volume: 2, Issue: 1
Submission: 26/12/2015; Accepted: 17/05/2016; Published: 24/05/2016
Abstract
Artery of Percheron (AOP) infarct is a diagnosis of high clinical and radiological suspicion due to early specific clinical and imaging findings related to the area involved by the infarct. The artery of Percheron is a rare variant artery of the posterior cerebral circulation which supplies blood to the bilateral paramedian thalami and the rostral midbrain. We report a case of a patient admitted in emergency with sudden onset loss of consciousness. A non-contrast CT scan of the head was performed, which revealed well defined hypodensity in bilateral paramedian thalamic region and along midbrain medially indicating an infarct in the territory of AOP.
Keywords: Artery of Percheron (AOP); Paramedian thalami and midbrain
Introduction
The thalamus is supplied by the various branches of posterior circulation and categorized into 4 territories: anterior, paramedian, inferolateral and posterior. The posterior thalamoperforating arteries branch off from the P1 segment of posterior cerebral artery and supply blood to the paramedian territory of the midbrain (paramedian arteries) [1]. Additionally, superior mesencephalic (or rubral) arteries that supply the rostral midbrain can branch separately from P1 or share a common origin with the paramedian arteries [2]. Thus, the paramedian arteries often supply the rostral midbrain. There are described normal variations of the neurovascular anatomy of the thalami and midbrain. Variation I is the most common, where each paramedian perforating artery arises from each left and right posterior cerebral artery. In variation IIb, the bilateral perforating thalamic arteries arise from one central artery called the artery of Percheron. which arises from the P1 segment of one posterior cerebral artery. Variant III is an arcade variant, with several small perforating branches arising from a single arterial arc that bridges the P1 segments of both posterior cerebral arteries. It supplies the paramedian thalami and the rostral midbrain [3,4]. Due to the type IIb variation any phenomenon causing occlusion of this single AOP will result in infarct involving midbrain and bilateral paramedian thalami.
Case Report
A 64-year-old right-handed man with sudden loss of consciousness is brought to the emergency department of the hospital. He also had a short history of memory impairment with normal motor functions. The first line of management is given with recording of vitals which show normal blood pressure and circulatory parameters. A head CT is performed along with other routine blood investigations. The blood investigations show normal results. The CT scan of head revealed a bilateral paramedian thalamic and midbrain hypodensity corresponding to an infarct in the territory of the artery of Percheron [Figure 1,Figure 2].
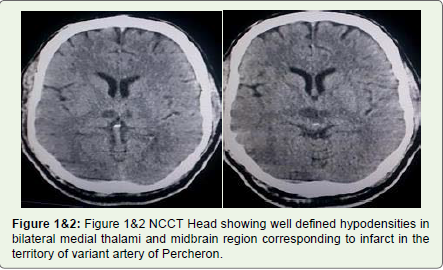
Figure 1&2: Figure 1&2 NCCT Head showing well defined hypodensities in bilateral medial thalami and midbrain region corresponding to infarct in the territory of variant artery of Percheron.
Discussion
The medial part of the thalamus is usually supplied by the paramedian arteries that arise from the first segment of posterior cerebral arteries on both sides. In about one third of humans, these arteries arise from a single artery known as the artery of Percheron (AOP) [5] which is too small to be visualised by MRA [6] and can only be detected on angiograms [7]. Also additionally due to normal variation this can supply rostral midbrain. Thus infarct in the territory of artery of Percheron will affect these areas. The three typical features of this stroke syndrome are altered mental status, memory impairment and the vertical gaze palsy [8]. Our patient presented with two out of the three typical features of this stroke syndrome, which are altered mental status and the memory impairment. The altered mental status is explained by involvement of reticular activating system [6] and the disrupted connections between the thalamus and the anterior orbitofrontal and medial prefrontal cortices. The thalamic structures which are involved in memory function are the mammillothalamic tract, anterior nucleus, and dorsomedial nucleus. The mammillothalamic tract and dorsomedial nucleus are supplied by the paramedian arteries and the anterior nucleus belongs to the polar territory. Amnesia appears to be more profound and persistent when lesions affect all of these structures [9]. The third feature of the triad is vertical gaze palsy, which is due to disruption of the cortical input that traverses the thalamus to reach the rostral interstitial medial longitudinal fasciculus. The main differential to AOP infarct is top of basilar artery syndrome which has more widespread distribution and other additional characteristics of posterior circulation infarcts [10], which is not present in our case.
Conclusion
The diagnosis may be delayed and the therapeutic window for thrombolytic therapy can be missed resulting in significant neurological impairment without knowledge about this normal variant artery and its supply. For patients presenting with altered mental status and memory impairment, vertical gaze palsy should be looked and consideration given to undertaking an urgent CT scan. The MRI with DWI sequencing can be done in order to diagnose AOP infarct when thrombolytic therapy might still be feasible. The distinct imaging pattern of ischemia helps in the early diagnosis of AOP infarct and management of the patients with thalamic strokes.
References
- Cosson A, Tatu L, Vuillier F, Parratte B, Diop M, et al. (2003) Arterial vascularization of the human thalamus: extra-parenchymal arterial groups. Surg Radiol Anat 25: 408-415.
- Bogousslavsky J, Regli F, Uske A (1988) Thalamic infarcts: clinical syndromes, etiology, and prognosis. Neurology 38: 837-848.
- Percheron G (1973) The anatomy of the arterial supply of the human thalamus and its use for the interpretation of the thalamic vascular pathology. Journal of Neurology 205: 1-13.
- Raphaeli G, Liberman A, Gomori J M, Steiner I (2006) Acute bilateral paramedian thalamic infarcts after occlusion of the artery of Percheron. Neurology 66: E7.
- López-Serna R, González-Carmona P, López-Martínez M (2009) Bilateral thalamic stroke due to occlusion of the artery of Percheron in a patient with patent foramen ovale: a case report. J Med Case Reports 3: 7392.
- Krampla W, Schmidbauer B, Hruby W (2008) Ischaemic stroke of the artery of Percheron (2007: 10b). Eur Radiol 18: 192-194.
- Kostanian V, Cramer SC (2007) Artery of Percheron thrombolysis. AJNR Am J Neuroradiol 28: 870-1.
- Lazzaro NA, Wright B, Castillo M, Fischbein NJ, Glastonbury CM, et al. (2010) Artery of Percheron infarction: imaging patterns and clinical spectrum. AJNR Am J Neuroradiol 31: 1283-9.
- Perren F, Clarke S, Bogousslavsky J (2005) The syndrome of combined polar and paramedian thalamic infarction. Arch Neurol 62: 1212-1216.
- Caplan LR (1980) “Top of the basilar” syndrome. Neurology 30: 72-79.