Case Report
Dyke-Davidoff-Masson Syndrome/ CerebralHemiatrophy in an Adult Male : A Rare Imaging Case
Seema Sharma*, Sohan Singh, Suman Bhagat, Harpreet Garcha
Corresponding author: Seema Sharma, Department of Radio Diagnosis and Imaging, Government Medical College,Amritsar, 143001, Phone Number-08146860055, Punjab, India Email: drgdsharda@gmail.com
Citation: Sharma S, Singh S, Bhagat S, Garcha H. Imaging in Disseminated Cysticercosis: A Case Report and Review of Literature. Indian J Appl02 Radiol. 2015;2(1): 107.
Copyright © 2016 Sharma S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Applied Radiology | Volume: 2, Issue: 1
Submission: 15/11/2015; Accepted: 28/03/2016; Published: 04/04/2016
Abstract
Dyke Davidoff Masson Syndrome (DDMS) is a rare condition characterized by seizures, hemiparesis/ hemiplegia, facial asymmetry and mental retardation. The underlying etiology is cerebral insult that may occur in uteroIor early in life. All modalities ableto image the brain (x ray skull, ultrasound, CT and MRI) will be able to more or less identify the key features, although MRI will give the best imaging. Radiologically, magnetic resonance (MR) and computed tomography (CT) shows the parenchymal abnormalities of unilateral loss of cerebral volume with ipsilateral ex vacuo dilatation of the lateral ventricle and sulci. There are compensatory bone alterations in the calvarium, such as thickening of the skull vault and enlargement of the paranasal sinusesand mastoid cells as well as elevation of the, orbital roof, petrous ridge and greater wing of the sphenoid bone. This occurs in adaptation to the relative vacuum created by the brain atrophy. Atrophy/hypoplasia of cerebral peduncle, basal ganglia, thalamus and cerebellum (ipsilateral or contra lateral hemisphere) may be present. In this case report, we discuss a case of twenty five year-old married male who presented with seizures, facial asymmetry, mental retardation and right -sided hemiparesis. Classical findings of the Dyke Davidoff Masson Syndrome were present on CT scan, so diagnosis was made on basis of the history, clinical features and radiological findings.
Keywords: Cerebral hemiatrohy; Hemiparesis; Seizures; Paranasal sinuses
Introduction
The Dyke-Davidoff-Masson Syndrome (DDMS) is defined as theatrophy or hypoplasia of one cerebral hemisphere (hemiatrophy) which is secondary to brain insult in fetal or early childhood period[1]. It is more common in males and in the left hemisphere [2]. It is characterized clinically by variable degrees of facial asymmetry, seizures, contralateral hemiplegia or hemiparesis, and mental retardation. Mental retardation is not always present and seizures may appear months or years after the onset of hemiparesis. CT/ MRI shows the parenchymal abnormalities of unilateral loss of cerebral volume with ipsilateral lateral ventricle dilatation, sulcal prominence with compensatory bone alterations in the calvarium, such asthickening, enlargement of the paranasal sinuses and mastoid cells aswell as elevation of the petrous ridge and greater wing of the sphenoidbone. Encephalomalacia, gliosis, porencephaly, loss of white and graymatter substance, hypoplastic cerebral peduncle and midline shift toward the atrophic side may also be present in the hemiatrophic brain [3,4]. There are only few cases of DDMS in the adult age group reported in literature to date. Here, we present a rare case of a 25 years old male who presented with seizures, facial asymmetry, mental retardation and right sided weakness and showed all the clinical and imaging features of the DDMS, so this diagnosis was considered.
Case Report
A 25-year-old married male was referred for CT scan with righthemiparesis and seizures. Past history revealed that he was a case ofpremature delivery (home) at eight months of gestation and delayed cry. There was h/o delayed milestones and mental retardation. He had first episode of seizures at about 2 years of age. Seizures were controlled with medication. Then he had seizure free interval of about 20 years.He has normal vision and hearing. Face asymmetry was appreciated. Now he again had an episode of generalized tonic clonic convulsions along with frothing and urinary incontinence after a long seizure free period and referred for CT scan. The CT brain of the present case showed atrophy of left cerebral hemisphere with dilatation of the left lateral ventricle [Figure 1] (Image A). There was falcine displacement towards the atrophic side with prominence of the left sulcal spaces and sylvian fissure (Image B). In the vault, we noted thickening of the frontal and parietal portion of the skull bones (Image C). There was enlargement of the left frontal sinus, sphenoid sinus and mastoid air cells (ImageD,E). There was elevation of the ipsilateral orbital roof and petrous ridge (Image F). These findings were consistent with the diagnosis of Dyke-Davidoff-Masson syndrome (DDMS). There was no need to recommend a Magnetic resonance scanning.
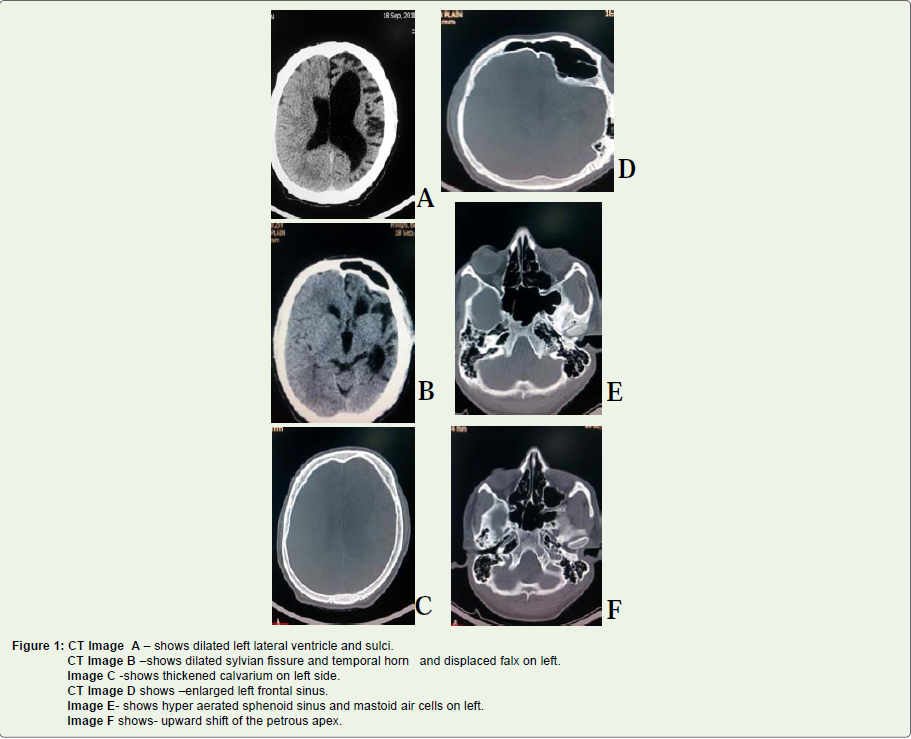
Figure 1: Figure 1: CT Image A - shows dilated left lateral ventricle and sulci.CT Image B - shows dilated sylvian fissure and temporal horn and displaced falx on left.Image C - shows thickened calvarium on left side.CT Image D shows - enlarged left frontal sinus.Image E - shows hyper aerated sphenoid sinus and mastoid air cells on left.Image F shows- upward shift of the petrous apex.
Discussion
Dyke-Davidoff-Masson syndrome was described as skull radiographic and pneumatoencephalographic changes in a series of 9patients whose clinical characteristics included hemiparesis, seizures, facial-asymmetry, and mental retardation in 1933 by Dyke-Davidoff and Masson [5].
Clinically it is characterized by seizures, facial asymmetry,contralateral hemiplegia or hemiparesis and mental retardation. However, mental retardation is not always present and seizures may appear months or years after the onset of hemi paresis. The clinical findings may be of variable degree according to the extent of the brain injury [1,6]. Both sexes and any of the hemispheres may be affected but male gender and left hemisphere involvement are more frequent [2]. This condition is usually diagnosed in childhood but rarely diagnosis can be made in teenagers and young adults [2].
The etiology of cerebral hemiatrophy may be classified into twogroups:
Congenital or Primary
Acquired or Secondary
In the congenital type, cerebral damage which usually has avascular origin, occurs during intrauterine life and symptoms appear at birth or shortly thereafter.
In the acquired or secondary type, cerebral insults occur duringthe perinatal period or later. The main etiologic factors involved aretrauma, infection, vascular abnormalities of the cerebral circulation,ischemic and hemorrhagic states, and in premature infants, subependymal germinal matrix and intraventricular haemorrhage [3,4]. In-utero gestational vascular occlusion involving middle cerebralvascular territory or coarctation of mid-aortic arch may decrease carotid arterial flow [1,7].
The involved hemisphere will have prominent sulcal spaces if thevascular insult occurs after birth or after sulcation is complete. On theother hand, if the vascular ischaemia occurs during intrauterine life,when the formation of gyri and sulci is incomplete, no prominentsulci will be present.
There may be variable extent of hypoplasia/atrophy of thecerebral peduncle, thalamus abnormal myelination and contralateral/ipsilateral cerebellar atrophy on the affected side. Encephalomalacia,gliosis, porencephaly, loss of white and gray matter substance, ipsilateral ventricular enlargement and midline shift may also be present in the hemiatrophic brain [3,4].
The brain reaches half of its adult size during the first year of life and reaches three-fourths of that size by the end of third year. As it enlarges, the brain presses outward on the bony tables and ispartly responsible for the gradual enlargement and general shape of the adult head. When the brain fails to grow properly, the other structures tend to direct their growth inward, thus accounting for the enlargement of the frontal sinus, the increased width of the diploic space and the elevations of the greater wing of sphenoid and the petrous ridge on the affected side [8]. These change can occur onlywhen brain damage is sustained before three years of age however, such changes may become evident as soon as nine-months after brain damage was sustained [9]. CT is preferred to conventionalradiography in DDMS as changes on skull plain radiographs may be so subtle and overlooked.
Shen et al., described three patterns of MRI showing cerebralhemiatrophy: MRI pattern I corresponds to diffuse cortical and subcortical atrophy; pattern II corresponds to diffuse cortical atrophycoupled with porencephalic cysts and pattern III corresponds to previous infarction with gliosis in middle cerebral artery territory [10].
Less common than ipsilateral cerebellar atrophy, contralateral or crossed cerebellar atrophy has also been described in the cerebral hemiatrophy syndrome and it is associated with long-standing, extensive and unilateral cerebral lesions with onset during infancy or early childhood [11].
Important differential diagnosis is Sturge Weber Syndrome,Rasmussen Encephalitis, Hemiconvulsion-Hemiplegia-Epilepsy Syndrome (HHE), Silver symdrome and some brain tumour [8,3]].
The treatment for DDMS is symptomatic and includesmanagement of seizures, hemiplegia or hemiparesis. The prognosis for the disease is better for patients who develop hemiparesis beyond the age of two years and also if there is no history of prolonged or recurrent seizures [12]. Children with intractable disabling seizures and hemiplegia are the potential candidates for hemispherectomy with a success rate of 85% in carefully selected cases [13].
In the present case, the classical features of the acquired type of cerebral hemiatrophy were found. The findings of dilated sulci and ventricle in the left hemisphere reflect a late onset of brain insult which was the consequence of premature delivery.
The prognosis in our patient is expected to be good as he had a long seizure free interval after the initial episode and that he was able to carry out his daily activities and functioning.
Conclusion
In conclusion, our case is one among the rare presentations ofacquired type of DDMS. The delayed clinical presentation in ourpatient was probably due to milder form of the disease. However theradiological features were classical of acquired type of DDMS. Imagingin addition to detailed history and thorough clinical examination insuch patients are crucial to arrive at the final diagnosis.
There is no conflicts of interest statement and funding
References
- Sharma S, Goyal D, Negi A, Sood RG, Jhobta A, et al. (2006) Indian Journal of Radiology & Imaging 16: 165- 166.
- Kumar S, Lakshmaiah V, Karthik Naidu KC (2011) A rare cause for seizures and mental retardation. Int J Biol Med Res 2: 1186 -1188.
- Sener RN, Jinkins JR (1992) MR of craniocerebral hemiatrophy. Clin Imaging16: 93-97.
- Zilkha A (1980) CT of cerebral hemiatrophy. AJR 135: 259-262.
- Dyke CG, Davidoff LM, Masson LB (1933) Cerebral hemiatrophy with homolateral hypertrophy of the skull and sinus. Surg Gynecol Obstet 57: 588- 600.
- Beena K, Narayanam RS (2010) Dyke-Davidoff Masson Syndrome. Velore. Imaging in Medicine. Annals Academy of Medicine 39: 6.
- Goyal J, Shah V, Rao S, Jindal N (2009) Dyke Davidoff Masson syndrome in Children. The Internet Journal of Pediatrics and Neonatology.
- Parker CE, Harris N, Mavalwala J (1972) Dyke-Davidoff-Masson syndrome: five case studies and deductions from dermatoglyphics. Clin Pediatr 11: 288- 292.
- Solomon G E, Hilal S K, Gold AP, Carter S (1970) Natural history of acute hemiplegia of childhood. Brain 93: 107-120.
- Shen WC, Chen CC, Lee SK, Ho YJ, Lee KR, et al. (1993) Magnetic resonance imaging of cerebral hemiatrophy. J Formos Med Assoc 92: 995- 1000.
- Carrazana EJ, Liu GT, Holmes GL (1992) Crossed cerebellar atrophy in the Dyke-Davidoff-Masson syndrome. Neuroradiology 34: 326-327.
- Jagadeeswaran G, Kumar VG, Saravanan T, Shanmuga Priya S (2013)Dyke Davidoff-Masson Syndrome in amiddle aged woman. Indian Journal ofMedical Case Reports 2: 34-37.
- Naraian NP, Kumar R, Narain B (2008) Dyke-Davidoff-Masson Syndrome. Indian Pediatr 45: 927-928.