Case Report
An Unusual Radiological Presentation of Invasive Adenocarcinoma of the Lung
Rajendran VR1*, Nuzair anzari2, Nimisha Rajendran3 and Dr Sathi PP4
1Professor and Head, Department of Radiodiagnosis, KMCT medical college, manassery, Mukkom, Kozhikode, India
2Senior resident, Department of Radiodiagnosis, KMCT medical college, Kozhikode, India
3Department of Radiodiagnosis, KMCT medical college, Kozhikode, India
4Professor and hod, Department of Pathology, KMCT medical college, Kozhikode, India
2Senior resident, Department of Radiodiagnosis, KMCT medical college, Kozhikode, India
3Department of Radiodiagnosis, KMCT medical college, Kozhikode, India
4Professor and hod, Department of Pathology, KMCT medical college, Kozhikode, India
*Corresponding author:Rajendran VR, Professor and Head, Department of Radiodiagnosis, KMCT medical college, manassery, Mukkom, Kozhikode, India. E-mail id: vrajendranclt@gmail.com
Copyright: © 2026 Rajendran VR, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information:Submission: 22/05/2026; Accepted: 25/06/2026; Published: 30/06/2026
Abstract
Bronchoalveolar carcinoma (subsumed under invasive adenocarcinoma according to 2015 classification of World Health Organization - WHO) typically presents asymptomatically, often as a solitary pulmonary nodule, and may remain unnoticed even as it disseminates. However, its presentation as nonresolving consolidation is rare. We report an unusual case of Bronchoalveolar carcinoma (BAC) in a young male, initially presenting with a productive
cough, exertional breathlessness, and multifocal bilateral consolidation on chest X-ray. Further evaluation with computed tomography (CT) of the chest and bronchoscopy confirmed the diagnosis of bronchoalveolar carcinoma.
In the ensuing case report, we present an uncommon case which highlights an atypical presentation of Bronchoalveolar carcinoma, masquerading as recurrent infections or tuberculosis & importance of considering it in differential diagnoses when confronted with persistent pulmonary consolidation.
Introduction
Bronchoalveolar carcinoma is an uncommon variant of lung
adenocarcinoma (subsumed under invasive adenocarcinoma
according to 2015 WHO classification) characterized by highly
variable clinical, radiographic, and histopathological features. It
occurs more frequently in non-smokers, women, and individuals of
Asian descent. Although classified under the spectrum of pulmonary
adenocarcinomas, it differs markedly in its presentation, therapeutic
approach, and overall prognosis, accounting for approximately 6.5%
of all primary lung neoplasms [1]
Bronchoalveolar carcinoma is derived from the epithelial cells located distally to the terminal bronchioles, and is defined as a primary lung cancer in peripheral locations. It is found growing in a lepidic (scale-like) manner near the alveolar septae without parenchymal, vascular, or pleural invasion [2]
Bronchoalveolar carcinoma is derived from the epithelial cells located distally to the terminal bronchioles, and is defined as a primary lung cancer in peripheral locations. It is found growing in a lepidic (scale-like) manner near the alveolar septae without parenchymal, vascular, or pleural invasion [2]
In most cases, Bronchoalveolar carcinoma presents as a peripheral
pulmonary nodule; however, it can also manifest as segmental or lobar
consolidation, and may exhibit a multifocal or diffuse distribution
pattern. [2,3]
Case Presentation:
A 31-year-old male nonsmoker presented with a five-year history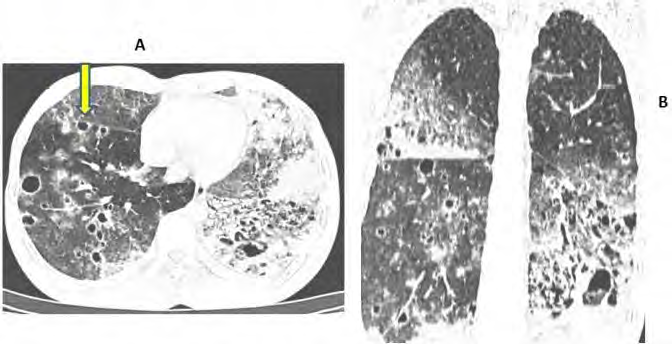
(2021–2025) of recurrent lower respiratory tract infections requiring
multiple hospital admissions, one of which led to a Cartridge-based
Nucleic Acid Amplification Test (CBNAAT) positive diagnosis of
pulmonary tuberculosis. He completed a year of Antitubercular
Therapy (ATT) with temporary clinical improvement, but continued
to experience recurrent symptoms. In his most recent admission
in 2025, respiratory complaints persisted despite a trial of broadspectrum
antibiotics.
Imaging Findings and Histopathological Evaluation:
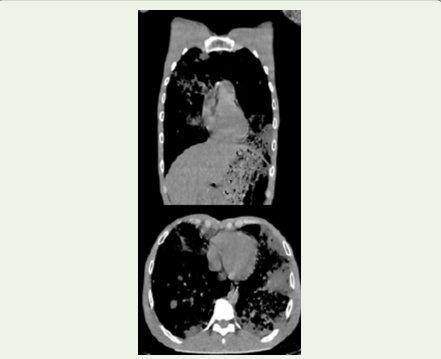
Sequential computed tomography imaging demonstrated
progressive ground-glass opacities involving both lung parenchyma
that initially spared the lingula of left upper lobe and right middle
lobe, later diffusely involving these segments.Subsequent scans revealed multiple cavitating nodules
with the striking “cheerios sign”, heightening suspicion for an
underlying malignancy in the setting of non-resolving pneumonia.
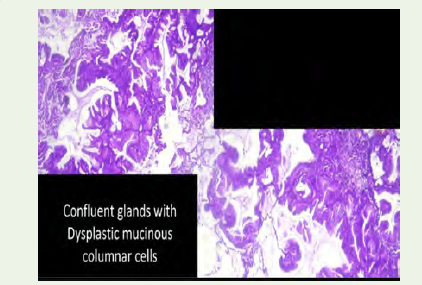
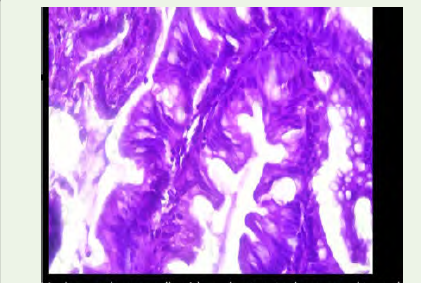
Histopathological evaluation of a lung biopsy confirmed invasive
mucinous adenocarcinoma with a predominant lepidic growth
pattern.
Discussion
In this entity, growth occurs along the alveolar septa and without
evidence of stromal, vascular or pleural invasion. Although only 4% of
lung cancers meet this definition, up to 20% of lung cancers comprise
a heterogeneous group of tumors with Bronchoalveolar carcinoma
histology mixed with a varying population of invasive cells, ranging
from predominant Bronchoalveolar carcinoma histology with a small
focus of invasion, to invasive adenocarcinoma with an isolated group
of cells with Bronchoalveolar carcinoma features at periphery [4]
Typically, three different radiological patterns are seen in Bronchoalveolar carcinoma: a solitary nodule or a mass of varying density, focal consolidation, or multifocal (diffuse) disease [5]
Typically, three different radiological patterns are seen in Bronchoalveolar carcinoma: a solitary nodule or a mass of varying density, focal consolidation, or multifocal (diffuse) disease [5]
Additionally, we have the Cheerios sign, described for the first
time by Reed and O’Neil in 1993, a rare computed tomography finding
characterized by a nodule with central radiolucency, resembling the
ring-shaped Cheerios breakfast cereal. It appears as a small, ring-like,
uniform shadow within otherwise normal lung tissue and results
from peribronchiolar proliferation of malignant cells, as seen in this
case [6]
Learning Point for Clinicians:
Clinicians are advised to maintain a heightened clinical vigilance
for bronchoalveolar carcinoma in patients presenting with persistent
or repetitive pulmonary consolidations refractory to antimicrobial
or anti-tubercular therapy, especially when imaging exhibits atypical
patterns such as multifocal opacities or the hallmark Cheerios sign, to
aid timely diagnosis and optimal therapeutic intervention.References
Citation
Rajendran VR, anzari N, Rajendran N, Sathi PP. An Unusual Radiological Presentation of Invasive Adenocarcinoma of the Lung. Indian J Appl Radiol. 2026;12(1): 236.