Case Report
Half a Breath: Radiologic Diagnosis of Pulmonary Aplasia in a Newborn
Swizzel Pereira* and De Sequeira Fernandes VMY
Department of Radiodiagnosis, Goa Medical College, Goa, India.
*Corresponding author:Dr. Swizzel Pereira, Department of Radiodiagnosis, Goa Medical College, Goa, India. E-mail id: swizzelpereira21@gmail.com
Copyright: ©2026 Pereira S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information:Submission: 18/04/2026; Accepted: 19/05/2026; Published: 23/05/2026
Abstract
Pulmonary aplasia is an extremely rare congenital anomaly characterized by the complete absence of unilateral lung parenchyma and vasculature, with a rudimentary, blind ending bronchus. In this case report, we present the clinical and radiological findings of a 1-day-old male neonate with respiratory distress since birth. Chest radiograph
revealed mediastinal shift towards the left side with hyperinflation of the right lung. Contrast-enhanced CT scan revealed the absence of the left lung, left pulmonary vessels, with a rudimentary, blind ending left main bronchus with marked ipsilateral cardio-mediastinal shift.
Keywords:Unilateral lung; Lung aplasia; Lung agenesis; Rudimentary bronchus
Introduction
Pulmonary aplasia is an extremely rare entity, having an incidence
of 0.0097% [1], most often occurring unilaterally, as bilateral
pulmonary aplasia is incompatible with life. It is characterised by
the absence of lung parenchyma, its vasculature, and the presence
of the rudimentary blind-ending bronchus. The presence of this
rudimentary bronchus is what differentiates this anomaly from
pulmonary agenesis. It is frequently associated with other congenital
abnormalities, mainly cardiovascular, and has been reported to occur
with the VACTERL syndrome [2].
Schneider [3] described the spectrum of congenital anatomical pulmonary abnormalities into three major types: (a) pulmonary agenesis, with complete absence of the lung, bronchus, or vascular supply on the affected side; (b) pulmonary aplasia, a rudimentary bronchus without pulmonary parenchyma; (c) pulmonary hypoplasia, a bronchus with varying amounts of pulmonary alveolar tissue extending from it. The case presented in this article is of the second type.
While aplasia of the lung may be suspected from the radiographic appearances, certain conditions must be excluded, such as pulmonary atelectasis, a plugged bronchus secondary to foreign body or mucous plugs, tumor, bronchiectasis, and stricture. For this reason, delineation of pulmonary anatomy with CT as well as investigation with bronchoscopy is essential.
Schneider [3] described the spectrum of congenital anatomical pulmonary abnormalities into three major types: (a) pulmonary agenesis, with complete absence of the lung, bronchus, or vascular supply on the affected side; (b) pulmonary aplasia, a rudimentary bronchus without pulmonary parenchyma; (c) pulmonary hypoplasia, a bronchus with varying amounts of pulmonary alveolar tissue extending from it. The case presented in this article is of the second type.
While aplasia of the lung may be suspected from the radiographic appearances, certain conditions must be excluded, such as pulmonary atelectasis, a plugged bronchus secondary to foreign body or mucous plugs, tumor, bronchiectasis, and stricture. For this reason, delineation of pulmonary anatomy with CT as well as investigation with bronchoscopy is essential.
Case Presentation
A 1-day-old male neonate presented with respiratory depression
since birth. The neonate was born at term by elective LSCS in view
of suspicion of cystic adenomatoid malformation on RADIUS scan.
Examination of the baby revealed an increased respiratory rate with
grunting and reduced SpO2. Breath sounds were absent over the left
hemithorax.
The baby required bag and mask ventilation at birth and was shifted to the neonatal intensive care unit with an endotracheal tube in situ, and later connected to a conventional ventilator.
A bedside chest radiograph revealed complete opacification of the left hemithorax with mediastinal shift to the right. The right lung appeared well aerated with herniation to the left side. (Figure1)
The baby required bag and mask ventilation at birth and was shifted to the neonatal intensive care unit with an endotracheal tube in situ, and later connected to a conventional ventilator.
A bedside chest radiograph revealed complete opacification of the left hemithorax with mediastinal shift to the right. The right lung appeared well aerated with herniation to the left side. (Figure1)
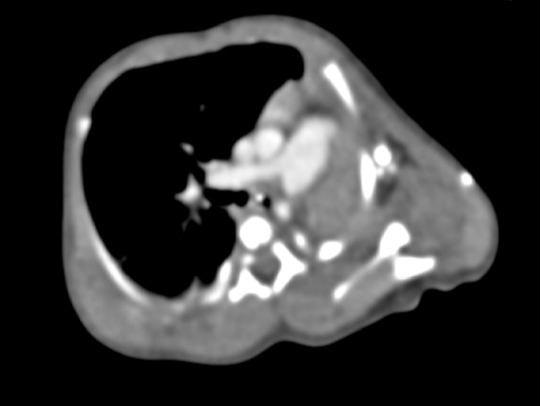
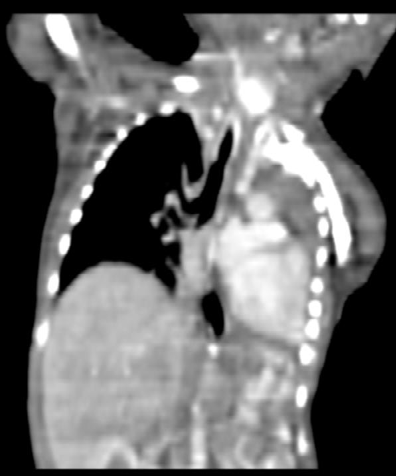
Subsequently performed contrast enhanced CT scan of the
thorax revealed non-visualization of the left lung parenchyma, the
left pulmonary vessels, and the presence of a small, blind ending,
rudimentary left main bronchus (Figure 2 and Figure 3). There was
a marked ipsilateral shift of the heart, thymus, and great vessels to
the left (Figure 4). Hyperinflation of the right lung with herniation
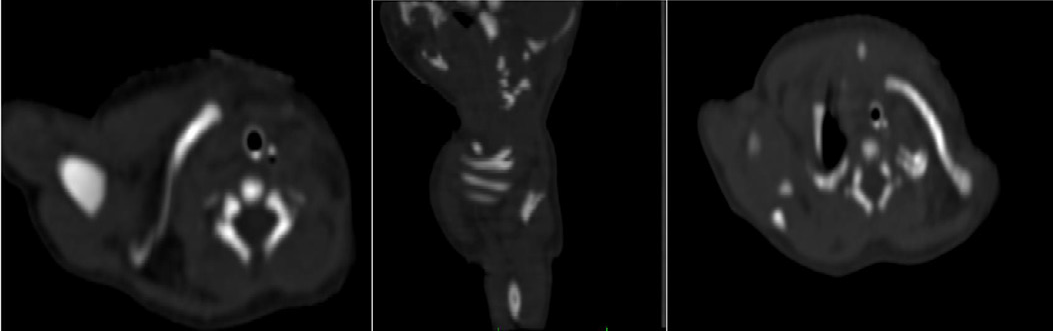
into the left hemithorax was noted (Figure 2 (b)). Additionally, bifid
appearance of the left 1st rib (Figure 5 (c)) as well as fusion of the
anterior ends of the left 1st and 2nd ribs (Figure 5 (b)) with narrowing
of the intervening intercostal spaces were noted. Bilateral cervical ribs
were also noted (Figure 5 (a)).
Levo-position of the heart with minimal pericardial effusion was
also noted.
2D echocardiography revealed the presence of a 3 mm-sized atrial
septal defect.


Discussion
Schneider’s 1912 classification, later modified by Boyden in 1955,
categorizes lung development anomalies into 3 types:
1. Type 1 (agenesis) - involves the complete absence of pulmonary structures;
2. Type 2 (aplasia) - includes a rudimentary bronchus without parenchyma; and
3. Type 3 (hypoplasia) presents with reduced lung cells, airways, and alveoli. The severity of hypoplasia is determined by the timing and nature of the insult during the pseudoglandular stage (5–17 weeks of gestation), a critical period when mechanical stimuli and pressure balance drive lung development. [4]
The exact underlying cause of pulmonary agenesis or aplasia is currently unclear; however, genetic, teratogenic, and mechanical factors are all thought to contribute.[7]
Lung formation starts in the foregut during the fourth and fifth weeks of gestation. Disruption in the symmetrical division of the bronchial primordium—possibly linked to aberrant blood flow in the dorsal aortic arch during this period—can cause one lung to be underdeveloped (hypoplasia), partially formed (aplasia), or entirely missing (agenesis). The contralateral lung then compensates by nearly doubling its alveolar production [8].
In lung aplasia, the tracheal bifurcation and carina play a key role by tethering the trachea to the pericardium and aortic arch. This attachment pulls the trachea along with the heart and major vessels. This tracheal shift leads to angulation and kinking just before its bifurcation and at the thoracic inlet, which narrows the airway. By comparison, lung agenesis lacks this bifurcation and its ligaments, avoiding such tracheal shifts and distortions [5].
Tracheal kinking and narrowing in the presence of the main bronchus stump disrupts laminar airflow and promotes turbulent flow dynamics. This increases airway resistance, expands dead space, and facilitates retention of bronchial secretions, thus increasing the risk of repeated respiratory infections. Normal diaphragm excursions further shift the mediastinum toward the low-pressure pleural space on the affected side. In left-sided aplasia, the right upper lobe’s anterior segment and middle lobe herniate, displacing the heart leftward, downward, and backward. Bronchial kinking leads to emphysema in these herniated segments, while compression from nearby vessels like the brachiocephalic arteries aggravates tracheal narrowing. The herniation thus reflects emphysematous expansion with poor perfusion, not genuine compensatory expansion [5].
Hemodynamic changes include compression of the superior vena cava and innominate vein, impairing cerebral venous drainage. Conditions like a patent foramen ovale or patent ductus arteriosus also promote left-to-right shunting, overloading the single working lung with extra blood volume. These factors drive early, worsening respiratory distress, often with infections in the remaining lung [5]. People with pulmonary agenesis, aplasia, or hypoplasia might show no symptoms or varying degrees of respiratory distress based on the extent of lung underdevelopment. In asymptomatic paediatric patients, these conditions are often an incidental finding. Lung agenesis often pairs with other birth defects, such as vertebral anomalies, cardiovascular defects, anorectal malformations, esophageal atresia, tracheoesophageal fistula, and genitourinary anomalies [5]. The presence of these associated anomalies negatively impacts the prognosis. In our case, the patient had a small atrial septal defect as well as skeletal anomalies.
Differential diagnosis includes pulmonary agenesis, pulmonary hypoplasia, atelectasis/collapse, and thoracic space-occupying lesions. The preferred imaging modality for a complete assessment of pulmonary aplasia (and other congenital anatomical pulmonary anomalies) is a contrast-enhanced CT scan. 3D reconstructions of blood vessels, airways, and pulmonary parenchyma accurately identify thoracic abnormalities and distinguish between lung agenesis, aplasia, and hypoplasia. Bronchoscopy can also confirm a short, rudimentary bronchus or rule out obstructions from foreign objects or mucus plugs.
In addition to vessel assessment, volume-rendered images can ensure virtual bronchoscopy to evaluate airways [10]. Pulmonary aplasia requires precise airway assessment for diagnosis and surgical planning. Virtual bronchoscopy excels here by clearly depicting bronchial absence or abrupt terminations. It offers high accuracy (up to 98%) in identifying tracheobronchial anomalies, correlating closely with gold-standard bronchoscopy [11]. Virtual bronchoscopy provides non-invasive, precise depiction of bronchial absence, aiding surgical planning and avoiding risks in infants, though it complements rather than replaces full CT assessment.
1. Type 1 (agenesis) - involves the complete absence of pulmonary structures;
2. Type 2 (aplasia) - includes a rudimentary bronchus without parenchyma; and
3. Type 3 (hypoplasia) presents with reduced lung cells, airways, and alveoli. The severity of hypoplasia is determined by the timing and nature of the insult during the pseudoglandular stage (5–17 weeks of gestation), a critical period when mechanical stimuli and pressure balance drive lung development. [4]
The exact underlying cause of pulmonary agenesis or aplasia is currently unclear; however, genetic, teratogenic, and mechanical factors are all thought to contribute.[7]
Lung formation starts in the foregut during the fourth and fifth weeks of gestation. Disruption in the symmetrical division of the bronchial primordium—possibly linked to aberrant blood flow in the dorsal aortic arch during this period—can cause one lung to be underdeveloped (hypoplasia), partially formed (aplasia), or entirely missing (agenesis). The contralateral lung then compensates by nearly doubling its alveolar production [8].
In lung aplasia, the tracheal bifurcation and carina play a key role by tethering the trachea to the pericardium and aortic arch. This attachment pulls the trachea along with the heart and major vessels. This tracheal shift leads to angulation and kinking just before its bifurcation and at the thoracic inlet, which narrows the airway. By comparison, lung agenesis lacks this bifurcation and its ligaments, avoiding such tracheal shifts and distortions [5].
Tracheal kinking and narrowing in the presence of the main bronchus stump disrupts laminar airflow and promotes turbulent flow dynamics. This increases airway resistance, expands dead space, and facilitates retention of bronchial secretions, thus increasing the risk of repeated respiratory infections. Normal diaphragm excursions further shift the mediastinum toward the low-pressure pleural space on the affected side. In left-sided aplasia, the right upper lobe’s anterior segment and middle lobe herniate, displacing the heart leftward, downward, and backward. Bronchial kinking leads to emphysema in these herniated segments, while compression from nearby vessels like the brachiocephalic arteries aggravates tracheal narrowing. The herniation thus reflects emphysematous expansion with poor perfusion, not genuine compensatory expansion [5].
Hemodynamic changes include compression of the superior vena cava and innominate vein, impairing cerebral venous drainage. Conditions like a patent foramen ovale or patent ductus arteriosus also promote left-to-right shunting, overloading the single working lung with extra blood volume. These factors drive early, worsening respiratory distress, often with infections in the remaining lung [5]. People with pulmonary agenesis, aplasia, or hypoplasia might show no symptoms or varying degrees of respiratory distress based on the extent of lung underdevelopment. In asymptomatic paediatric patients, these conditions are often an incidental finding. Lung agenesis often pairs with other birth defects, such as vertebral anomalies, cardiovascular defects, anorectal malformations, esophageal atresia, tracheoesophageal fistula, and genitourinary anomalies [5]. The presence of these associated anomalies negatively impacts the prognosis. In our case, the patient had a small atrial septal defect as well as skeletal anomalies.
Differential diagnosis includes pulmonary agenesis, pulmonary hypoplasia, atelectasis/collapse, and thoracic space-occupying lesions. The preferred imaging modality for a complete assessment of pulmonary aplasia (and other congenital anatomical pulmonary anomalies) is a contrast-enhanced CT scan. 3D reconstructions of blood vessels, airways, and pulmonary parenchyma accurately identify thoracic abnormalities and distinguish between lung agenesis, aplasia, and hypoplasia. Bronchoscopy can also confirm a short, rudimentary bronchus or rule out obstructions from foreign objects or mucus plugs.
In addition to vessel assessment, volume-rendered images can ensure virtual bronchoscopy to evaluate airways [10]. Pulmonary aplasia requires precise airway assessment for diagnosis and surgical planning. Virtual bronchoscopy excels here by clearly depicting bronchial absence or abrupt terminations. It offers high accuracy (up to 98%) in identifying tracheobronchial anomalies, correlating closely with gold-standard bronchoscopy [11]. Virtual bronchoscopy provides non-invasive, precise depiction of bronchial absence, aiding surgical planning and avoiding risks in infants, though it complements rather than replaces full CT assessment.
The prognosis depends on the degree of underdevelopment and
the severity of any associated congenital anomalies.
In children with lung aplasia, mortality reaches 33% in the
first year and 50% within five years. Fatalities typically stem from
infections in the single lung combined with major heart and vascular
defects [6]. Survivors past five years without severe infections can
often expect a near-normal lifespan [9].
Intrauterine diagnosis of pulmonary aplasia relies on meticulous assessment of the fetal thorax with ultrasound. These features include the absence of lung tissue on the affected side, where normal echogenic lung tissue cannot be identified, with ipsilateral shift of the mediastinal structures. This feature is key to differentiating from other pulmonary anomalies like CCAM and CDH, which would lead to contralateral mediastinal shift. Other secondary features would include rotation of the cardiac axis, oligohydramnios or polyhydramnios, inability to demonstrate ipsilateral pulmonary vascular structures on doppler study, and various skeletal anomalies. Fetal MRI may play a role in the quantification of the contralateral lung volume. Management focuses on preventing recurrent infections, using symptom-relief measures like expectorants and bronchodilators, and management of other complications. Prophylactic vaccines or treatments for respiratory syncytial virus, pneumococcus, and influenza are advised. Asymptomatic cases need no intervention. For those with a bronchial stump (hypoplastic bud), surgery to remove it may be necessary if postural drainage and antibiotics don’t clear infections [7]. Surgical translocation of the ipsilateral diaphragm can decrease the morbidity and mortality of children with pulmonary aplasia [5]
Intrauterine diagnosis of pulmonary aplasia relies on meticulous assessment of the fetal thorax with ultrasound. These features include the absence of lung tissue on the affected side, where normal echogenic lung tissue cannot be identified, with ipsilateral shift of the mediastinal structures. This feature is key to differentiating from other pulmonary anomalies like CCAM and CDH, which would lead to contralateral mediastinal shift. Other secondary features would include rotation of the cardiac axis, oligohydramnios or polyhydramnios, inability to demonstrate ipsilateral pulmonary vascular structures on doppler study, and various skeletal anomalies. Fetal MRI may play a role in the quantification of the contralateral lung volume. Management focuses on preventing recurrent infections, using symptom-relief measures like expectorants and bronchodilators, and management of other complications. Prophylactic vaccines or treatments for respiratory syncytial virus, pneumococcus, and influenza are advised. Asymptomatic cases need no intervention. For those with a bronchial stump (hypoplastic bud), surgery to remove it may be necessary if postural drainage and antibiotics don’t clear infections [7]. Surgical translocation of the ipsilateral diaphragm can decrease the morbidity and mortality of children with pulmonary aplasia [5]
Conclusion
Pulmonary aplasia is a rare congenital anomaly that should be
considered in neonates presenting with unilateral opaque hemithorax
and mediastinal shift. Imaging, in particular CECT, plays a pivotal
role in definitive diagnosis by demonstrating the absence of lung
parenchyma, bronchial anatomy, and vascular structures. Early
diagnosis enables appropriate clinical management and evaluation
for associated anomalies.
References
Citation
Pereira S, De Sequeira Fernandes VMY. Half a Breath: Radiologic Diagnosis of Pulmonary Aplasia in a Newborn. Indian J Appl Radiol. 04 2026;12(1): 235.