Case Report
An Incidental Case of Duplicated Inferior Vena Cava with Dorsal Pancreatic Agenesis- A Case Report
Siripurapu Vinaya Ratna*, Achala Shravya G, Siddharth Pandey, Shiva Shankaran and Vidhya Rani R
Department of Radiodiagnosis, Sapthagiri Institute of Medical Sciences and Research Centre, Bangalore, Karnataka, India.
*Corresponding author:Dr. Siripurapu Vinaya Ratna, Department of Radiodiagnosis, Sapthagiri Institute of Medical Sciences and Research Centre, Bangalore, Karnataka, India. E-mail Id: vinaya.siripurapu12@gmail.com
Copyright: © 2026 Vinaya SR, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information:Submission: 08/03/2026; Accepted: 05/05/2026; Published: 09/05/2026
Abstract
Duplicated inferior vena cava (IVC) and dorsal pancreatic agenesis are rare congenital anomalies that are most often detected incidentally on crosssectional imaging. The coexistence of these two anomalies is exceedingly uncommon and may have important diagnostic and procedural implications. We report a case of a 17-year-old female who presented with diffuse abdominal pain and was incidentally found to have a duplicated IVC and dorsal pancreatic agenesis on contrast-enhanced computed tomography (CT). Recognition of such congenital vascular and pancreatic anomalies is essential to avoid diagnostic pitfalls and to prevent potential complications during surgical or interventional procedures. This case highlights the importance of meticulous evaluation of cross-sectional imaging for identifying rare congenital variants and understanding their potential associations.
Keywords:Incidental Association; Duplicated IVC; Dorsal Pancreatic Agenesis; Computed Tomography.
Introduction
The inferior vena cava (IVC) is the major venous channel
that carries deoxygenated blood from the lower limbs, pelvic
region and abdomen back to the right atrium of the heart [1].Its
formation occurs between the sixth and tenth weeks of gestation
through a complex process of anastomosis and regression of several
embryonic veins, especially the cardinal and subcardinal veins [7].
Disruptions or variations in this developmental process may result
in IVC anomalies, the most frequent being a subrenal duplicated IVC
(DIVC), with a reported prevalence of approximately 0.2%–3% in the
general population [5].
Subrenal DIVC arises due to the persistence of both posterior
cardinal veins, which subsequently join at the lumbar or thoracic
level to form a single IVC [1]. Based on the site of this confluence,
subrenal DIVC is classified into two types: type I, where the union
occurs above the renal veins, and type II, where it occurs below the
renal veins [7].
Duplication of the IVC is an uncommon anatomical variation that is typically asymptomatic and is often discovered incidentally on imaging studies conducted for other clinical reasons [2]. Recognition of this vascular anomaly is clinically important, particularly in patients undergoing abdominal or retroperitoneal surgery and vascular interventions, as failure to identify a duplicated IVC may result in diagnostic pitfalls or inadvertent vascular injury [2].
Dorsal pancreatic agenesis is a rare congenital condition marked by the partial or complete absence of the pancreatic body and tail, resulting from incomplete development of the dorsal pancreatic bud [3]. Although many patients remain asymptomatic, the condition may occasionally present with abdominal pain, recurrent pancreatitis, or disturbances in glucose metabolism [4].
The coexistence of duplicated IVC and dorsal pancreatic agenesis is exceedingly rare, with only a limited number of reports describing pancreatic or systemic anomalies associated with IVC variants in the literature [6]. We report a case of incidental detection of duplicated IVC and dorsal pancreatic agenesis in a young female undergoing radiological evaluation for abdominal pain.
From a radiological perspective, this case highlights the importance of a systematic and comprehensive evaluation of abdominal anatomy. Identification of a duplicated IVC should prompt careful assessment of venous anatomy, including the level of confluence and its relationship to the renal veins, which is critical for surgical and interventional planning [2]. Similarly, recognition of dorsal pancreatic agenesis should lead to evaluation for associated complications and differentiation from mimics [3].
Duplication of the IVC is an uncommon anatomical variation that is typically asymptomatic and is often discovered incidentally on imaging studies conducted for other clinical reasons [2]. Recognition of this vascular anomaly is clinically important, particularly in patients undergoing abdominal or retroperitoneal surgery and vascular interventions, as failure to identify a duplicated IVC may result in diagnostic pitfalls or inadvertent vascular injury [2].
Dorsal pancreatic agenesis is a rare congenital condition marked by the partial or complete absence of the pancreatic body and tail, resulting from incomplete development of the dorsal pancreatic bud [3]. Although many patients remain asymptomatic, the condition may occasionally present with abdominal pain, recurrent pancreatitis, or disturbances in glucose metabolism [4].
The coexistence of duplicated IVC and dorsal pancreatic agenesis is exceedingly rare, with only a limited number of reports describing pancreatic or systemic anomalies associated with IVC variants in the literature [6]. We report a case of incidental detection of duplicated IVC and dorsal pancreatic agenesis in a young female undergoing radiological evaluation for abdominal pain.
From a radiological perspective, this case highlights the importance of a systematic and comprehensive evaluation of abdominal anatomy. Identification of a duplicated IVC should prompt careful assessment of venous anatomy, including the level of confluence and its relationship to the renal veins, which is critical for surgical and interventional planning [2]. Similarly, recognition of dorsal pancreatic agenesis should lead to evaluation for associated complications and differentiation from mimics [3].
Case Report
A 17-year-old female presented with diffuse, intermittent,
non-radiating abdominal pain of several weeks’ duration. There
was no history of trauma, fever, vomiting, jaundice, or urinary
symptoms. Physical examination was unremarkable and laboratory
investigations, including liver function tests and pancreatic enzymes,
were within normal limits.
Ultrasonography of the abdomen was performed as the initial imaging modality. The pancreatic head was visualized and appeared normal; however, the body and tail of the pancreas could not be adequately assessed due to overlying bowel gas. No other significant abnormalities were detected on ultrasound examination.
Contrast-enhanced computed tomography (CECT) of the abdomen and pelvis was performed, demonstrating two separate infrarenal IVC segments located on either side of the abdominal aorta. The left infrarenal IVC drained the left common iliac vein and
Ultrasonography of the abdomen was performed as the initial imaging modality. The pancreatic head was visualized and appeared normal; however, the body and tail of the pancreas could not be adequately assessed due to overlying bowel gas. No other significant abnormalities were detected on ultrasound examination.
Contrast-enhanced computed tomography (CECT) of the abdomen and pelvis was performed, demonstrating two separate infrarenal IVC segments located on either side of the abdominal aorta. The left infrarenal IVC drained the left common iliac vein and
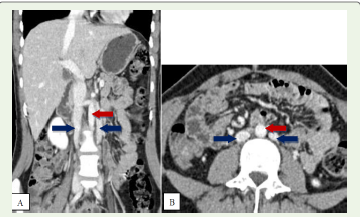


continued superiorly to join the left renal vein, which then crossed
anterior to the aorta to join the right suprarenal IVC, consistent with
typical duplicated IVC anatomy.
There was no evidence of azygous continuation or interruption of the hepatic segment of the IVC. Both infrarenal IVC segments appeared symmetrical in calibre.
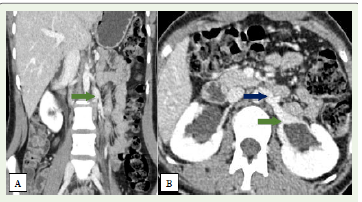
CT imaging also revealed absence of the pancreatic body and tail, with preservation of the pancreatic head and uncinate process, consistent with dorsal pancreatic agenesis. No evidence of pancreatic inflammation, duct dilatation, or peripancreatic fluid collection was identified.
No other associated congenital anomalies were detected. The patient was managed conservatively and counselled regarding the incidental findings. No immediate intervention was required, and clinical follow-up was advised.
There was no evidence of azygous continuation or interruption of the hepatic segment of the IVC. Both infrarenal IVC segments appeared symmetrical in calibre.
CT imaging also revealed absence of the pancreatic body and tail, with preservation of the pancreatic head and uncinate process, consistent with dorsal pancreatic agenesis. No evidence of pancreatic inflammation, duct dilatation, or peripancreatic fluid collection was identified.
No other associated congenital anomalies were detected. The patient was managed conservatively and counselled regarding the incidental findings. No immediate intervention was required, and clinical follow-up was advised.
Discussion
Duplication of the IVC is an uncommon congenital vascular
anomaly, with a reported prevalence ranging from 0.2% to 3% in
the general population. It results from the persistence of both right
and left supracardinal veins during embryogenesis, rather than the
normal regression of the left-sided venous system [1]. In most cases,
this anomaly is clinically silent and detected incidentally on imaging.
Recognition is important in radiological and surgical practice,
as failure to identify a duplicated IVC may lead to complications
during retroperitoneal surgery, renal transplantation, or vascular
interventions, including inadvertent vascular injury or significant
bleeding [7]. Additionally, duplicated IVC can mimic para-aortic
lymphadenopathy or retroperitoneal masses, potentially causing
diagnostic errors if unrecognized [5].
Dorsal pancreatic agenesis results from failure of development of the dorsal pancreatic bud [3]. Cross-sectional imaging, particularly contrast-enhanced CT, is crucial for diagnosis, typically showing absence of the pancreatic body and tail while the head and uncinate process remain intact [6]. It is important to differentiate this congenital anomaly from acquired conditions such as pancreatic atrophy or fatty replacement. Some patients may present with abdominal pain, pancreatitis, or diabetes mellitus due to reduced islet cell mass [4].
The coexistence of duplicated IVC and dorsal pancreatic agenesis is exceedingly rare, reflecting a potential shared disturbance in embryological mesodermal development [4]. Prior reports have described associations between IVC anomalies and pancreatic developmental abnormalities, including pancreatic divisum, as well as other congenital anomalies such as duplicated renal systems [2].
Our case adds to the limited literature documenting this rare association. Unlike previously reported cases with additional congenital anomalies or clinical manifestations, our patient presented with nonspecific abdominal pain, and both anomalies were incidentally detected. This supports prior observations that such congenital variants are often clinically silent and increasingly recognized due to widespread use of advanced imaging techniques.
Dorsal pancreatic agenesis results from failure of development of the dorsal pancreatic bud [3]. Cross-sectional imaging, particularly contrast-enhanced CT, is crucial for diagnosis, typically showing absence of the pancreatic body and tail while the head and uncinate process remain intact [6]. It is important to differentiate this congenital anomaly from acquired conditions such as pancreatic atrophy or fatty replacement. Some patients may present with abdominal pain, pancreatitis, or diabetes mellitus due to reduced islet cell mass [4].
The coexistence of duplicated IVC and dorsal pancreatic agenesis is exceedingly rare, reflecting a potential shared disturbance in embryological mesodermal development [4]. Prior reports have described associations between IVC anomalies and pancreatic developmental abnormalities, including pancreatic divisum, as well as other congenital anomalies such as duplicated renal systems [2].
Our case adds to the limited literature documenting this rare association. Unlike previously reported cases with additional congenital anomalies or clinical manifestations, our patient presented with nonspecific abdominal pain, and both anomalies were incidentally detected. This supports prior observations that such congenital variants are often clinically silent and increasingly recognized due to widespread use of advanced imaging techniques.
Conclusion
This case highlights the rare incidental coexistence of a duplicated
IVC and dorsal pancreatic agenesis in a young patient evaluated
for abdominal pain. Recognition of such anomalies is clinically
important to prevent diagnostic errors and to guide safe surgical or
interventional planning. Radiologists and clinicians should maintain
a high index of suspicion for additional congenital anomalies
whenever a variant is identified, as comprehensive evaluation can
have significant implications for patient management.
References
Citation
Vinaya SR, Shravya AG, Pandey S, Shankaran S, Vidhya RR. An Incidental Case of Duplicated Inferior Vena Cava with Dorsal Pancreatic Agenesis- A Case Report. Indian J Appl Radiol. 2026;12(1): 234.