Case Report
MRI Diagnosis of OHVIRA Syndrome in Adulthood: A Case Report
Achala Shravya G, Siripurapu Vinaya Ratna, Vidhya Rani R and Siddharth Pandey*
Department of Radiodiagnosis, Sapthagiri Institute of Medical Sciences and Research Centre, Bangalore, Karnataka, India
*Corresponding author:Dr. Siddharth Pandey, Department of Radiodiagnosis, Sapthagiri Institute of Medical Sciences and Research Centre, Bangalore, Karnataka, India. E-mail Id: sidd110798@gmail.com
Copyright: © 2026 Shravya GA, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information: Submission: 07/03/2026; Accepted: 27/04/2026; Published: 30/04/2026
Abstract
Obstructed hemivagina with ipsilateral renal anomaly (OHVIRA) syndrome is a rare congenital Müllerian duct anomaly. It is classically characterized by the presence of uterus didelphys, an obstructed hemivagina, and absence of the kidney on the same side (ipsilateral renal agenesis). Symptoms typically begin soon after menarche; however, delayed presentation into adulthood is very rare and may results in diagnostic confusion. Magnetic resonance imaging
(MRI) of the pelvis plays a crucial role in clearly mapping the anatomy in detail, enabling an accurate diagnosis and providing valuable guidance for surgical planning. Here we are describing a rare case of OHVIRA syndrome with a delayed presentation at 23-years of age, highlighting the MRI features which plays a crucial role in definitive diagnosis.
Keywords:OHVIRA syndrome; delayed presentation; Müllerian duct anomaly; uterus didelphys; MRI pelvis
Introduction
Congenital malformations of the female genital tract consist of
a group of miscellaneous deviations from normal anatomy. During
embryogenesis abnormal development, fusion, or resorption of
the paramesonephric ducts leads to Müllerian duct anomalies [1].
OHVIRA syndrome, also known as Herlyn–Werner–Wunderlich
syndrome, is a rare variant, characterized by triad of uterus didelphys,
unilateral obstructed hemivagina and ipsilateral renal anomaly
[2]. The incidence of this syndrome is low, and it often remains
underdiagnosed. The incidence of OHVIRA syndrome varies from
0.1% to 3.8% [3]
Most patients present soon after menarche with cyclical pelvic pain, dysmenorrhea, or pelvic mass due to accumulation of menstrual blood in the obstructed hemivagina [4]. However, in some cases symptoms may be subtle or intermittent, leading to delayed presentation into adulthood. Such delayed diagnosis poses a significant clinical challenge, as menstruation from the unobstructed side may mask the underlying anomaly [5].
Most patients present soon after menarche with cyclical pelvic pain, dysmenorrhea, or pelvic mass due to accumulation of menstrual blood in the obstructed hemivagina [4]. However, in some cases symptoms may be subtle or intermittent, leading to delayed presentation into adulthood. Such delayed diagnosis poses a significant clinical challenge, as menstruation from the unobstructed side may mask the underlying anomaly [5].
Imaging plays a central role in the evaluation of suspected
Müllerian anomalies. While ultrasonography serves as an initial
screening tool, MRI is widely regarded as the gold standard because
it provides exceptional soft-tissue detail and allows images to be
viewed in multiple planes, giving a clearer and more comprehensive
understanding of the anatomy [4]. This report describes a case
of OHVIRA syndrome with delayed presentation in a 23-yearold
female, emphasizing the importance of radiologic evaluation,
particularly MRI, in atypical presentations.
Case Report
A 23-year-old female presented with a history of pain abdomen
and white discharge since last one month. The pain was gradually
progressive in nature. Menstrual cycles were regular, and there was
no history of amenorrhea, which likely contributed to delayed clinical
suspicion.
Initial pelvic ultrasonography was performed, which suggested the presence of a Müllerian duct anomaly with a fluid-filled structure adjacent to the uterus. Bilateral ovaries appeared normal in size and echotexture. To further characterize the findings, the patient was referred for MRI pelvis.
MRI was performed using multiplanar T1-weighted, T2- weighted, and fat-suppressed sequences. Normal morphology and signal characteristics of both ovaries noted on ultrasound was subsequently confirmed on MRI.
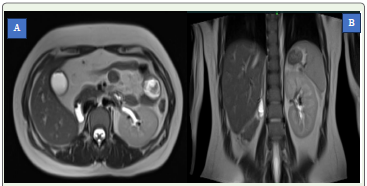
Additionally, screening images of the abdomen demonstrated absence of the right kidney, confirming ipsilateral renal agenesis. Based on these characteristic findings, a diagnosis of OHVIRA syndrome was established.
Initial pelvic ultrasonography was performed, which suggested the presence of a Müllerian duct anomaly with a fluid-filled structure adjacent to the uterus. Bilateral ovaries appeared normal in size and echotexture. To further characterize the findings, the patient was referred for MRI pelvis.
MRI was performed using multiplanar T1-weighted, T2- weighted, and fat-suppressed sequences. Normal morphology and signal characteristics of both ovaries noted on ultrasound was subsequently confirmed on MRI.
Additionally, screening images of the abdomen demonstrated absence of the right kidney, confirming ipsilateral renal agenesis. Based on these characteristic findings, a diagnosis of OHVIRA syndrome was established.
Imaging Findings:
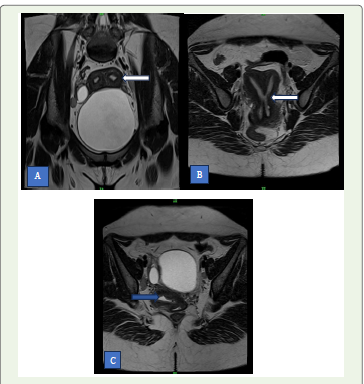
MRI: Axial and sagittal T2-weighted images demonstrated uterus
didelphys, with two separate uterine horns and cervices. The right
hemivagina was markedly distended, showing T1 hyperintense and
T2 heterogeneous signal intensity, consistent with hematocolpos
secondary to obstructed hemivagina. The left hemivagina appeared
patent and normal. Coronal abdominal images revealed absence
of the right kidney, confirming ipsilateral renal agenesis. These
combined findings were diagnostic of OHVIRA syndrome.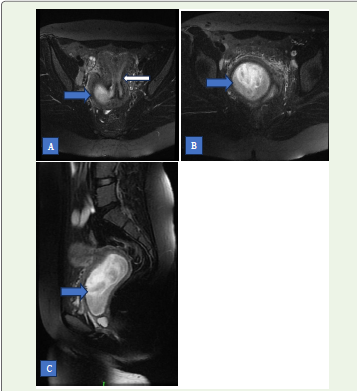
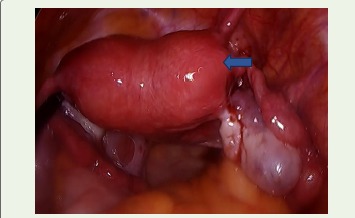
Patient underwent laparoscopic colpotomy. Post procedural
Ultrasound and MRI showed reduction in the right hemi-vaginal
collection (hematocolpos). After 2 weeks vaginoplasty was done.
Discussion
Female reproductive function depends on the intact genital
tract along with a functional hypothalamic–pituitary–ovarian axis.
Aberration in any of the systems may significantly affect a woman’s
reproductive potential, thereby negatively affecting her quality of life
[2]. OHVIRA syndrome develops due to a disruption in early fetal
development, around the 8th week of gestation, when the Müllerian
and mesonephric ducts fail to develop and fuse normally [2]. When the
mesonephric duct does not develop properly, the kidney on the same
side may fail to form (ipsilateral renal agenesis). At the same time,
abnormal development of the Müllerian ducts can lead to duplication
of the uterus along with obstruction of one side of the vagina [4].
OHVIRA or Herlyn-Werner-Wunderlich (HWW) syndrome is
characterised by a triad of type III Müllerian duct anomaly (uterus
didelphys), obstructed hemivagina and mesonephric duct anomalies
[6].
Although the classical presentation occurs during adolescence shortly after menarche, delayed diagnosis into adulthood, as seen in this case, is rare. Such delay may occur due to: partial vaginal obstruction, gradual accumulation of menstrual blood, regular menstruation from the unobstructed hemivagina and mild or nonspecific symptoms [5]. The role of imaging is fundamental in the evaluation of suspected cases. Ultrasound is usually the initial imaging method because it is easily available and non-invasive. However, it can sometimes fall short when it comes to clearly defining complex pelvic anatomy. MRI is generally preferred because it provides outstanding soft-tissue detail and allows images to be viewed in multiple planes. This makes it especially helpful for clearly outlining the shape and structure of the uterus, pinpointing the exact level and cause of vaginal obstruction, assessing the nature of any retained fluid or blood, and identifying associated renal abnormalities [4]. Early and accurate radiologic diagnosis is essential to prevent complications such as endometriosis, pelvic adhesions, infection, and infertility. This is particularly important in patients with delayed presentation, where prolonged obstruction may result in significant morbidity.
Although the classical presentation occurs during adolescence shortly after menarche, delayed diagnosis into adulthood, as seen in this case, is rare. Such delay may occur due to: partial vaginal obstruction, gradual accumulation of menstrual blood, regular menstruation from the unobstructed hemivagina and mild or nonspecific symptoms [5]. The role of imaging is fundamental in the evaluation of suspected cases. Ultrasound is usually the initial imaging method because it is easily available and non-invasive. However, it can sometimes fall short when it comes to clearly defining complex pelvic anatomy. MRI is generally preferred because it provides outstanding soft-tissue detail and allows images to be viewed in multiple planes. This makes it especially helpful for clearly outlining the shape and structure of the uterus, pinpointing the exact level and cause of vaginal obstruction, assessing the nature of any retained fluid or blood, and identifying associated renal abnormalities [4]. Early and accurate radiologic diagnosis is essential to prevent complications such as endometriosis, pelvic adhesions, infection, and infertility. This is particularly important in patients with delayed presentation, where prolonged obstruction may result in significant morbidity.
Conclusion
OHVIRA syndrome, though rare, has characteristic imaging
features that allow definitive diagnosis. MRI plays a crucial role in
accurately identifying uterovaginal anatomy, detecting hematocolpos
and demonstrating associated renal anomalies. Awareness of this
condition and careful evaluation with pelvic MRI in young females
presenting with cyclical pelvic pain can facilitate early diagnosis and
appropriate surgical management, thereby improving long-term
reproductive outcomes.
Learning Points:
• Delayed presentation of OHVIRA syndrome can occur in
adulthood due to partial obstruction or gradual accumulation
of menstrual blood.• MRI is the gold standard imaging modality for accurate diagnosis and preoperative anatomical delineation.
• Identification of ipsilateral renal anomaly should prompt careful evaluation for associated Müllerian duct anomalies. • Early radiologic diagnosis is essential to prevent complications such as endometriosis, pelvic adhesions and infertility.
References
Citation
Shravya GA, Ratna SV, Rani RV, Pandey S. MRI Diagnosis of OHVIRA Syndrome in Adulthood: A Case Report. Indian J Appl Radiol. 2026;12(1): 232.