Case Report
ECG-Gated High Resolution CT Evaluation of a Ruptured Non-Coronary Sinus of Valsalva Aneurysm Draining into the Right Atrium: A Case Report
Vaisakh Ajith1*, Chandresh Karnavat2 and Shrinivas B. Desai3
1DNB Radiology Resident, Jaslok Hospital and Research Centre, Mumbai, India
2Consultant Radiologist, Jaslok Hospital and Research Centre, Mumbai, India
3Head of Radiology Department, Jaslok Hospital and Research Centre, Mumbai, India
2Consultant Radiologist, Jaslok Hospital and Research Centre, Mumbai, India
3Head of Radiology Department, Jaslok Hospital and Research Centre, Mumbai, India
*Corresponding author:Dr. Vaisakh Ajith, Department of Radiology Jaslok Hospital and Research Centre15, Dr. G. Deshmukh Marg, Mumbai, Maharashtra, India. E-mail Id: vaisakhsrt@gmail.com
Copyright: ©2026 Ajith V, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information: Submission: 26/02/2026; Accepted: 15/04/2026; Published: 18/04/2026
Abstract
Background: Rupture of a sinus of Valsalva aneurysm (SOVA) is an uncommon but potentially life-threatening condition requiring prompt diagnosis and surgical intervention. While echocardiography is often used as an initial screening modality, computed tomography (CT) provides superior anatomical delineation and is invaluable for surgical planning.
Case Presentation: A 41-year-old female presented with rapidly progressive dyspnea and orthopnea with features of cardiac decompensation. ECGgated CT aortography revealed a focal aneurysmal dilatation of the non-coronary sinus of Valsalva with a rupture tract communicating into the right atrium. The aneurysmal sac was seen protruding into the right atrium with indentation of the adjacent tricuspid valve leaflet. Associated right-sided chamber dilatation and signs of pulmonary hypertension were noted. The patient subsequently underwent surgical repair, and intraoperative findings correlated with CT imaging.
Conclusion: ECG-gated CT angiography provides precise localization of the rupture site, delineation of the fistulous tract, and assessment of valvular involvement, thereby playing a crucial role in preoperative planning of ruptured sinus of Valsalva aneurysms.
Case Presentation: A 41-year-old female presented with rapidly progressive dyspnea and orthopnea with features of cardiac decompensation. ECGgated CT aortography revealed a focal aneurysmal dilatation of the non-coronary sinus of Valsalva with a rupture tract communicating into the right atrium. The aneurysmal sac was seen protruding into the right atrium with indentation of the adjacent tricuspid valve leaflet. Associated right-sided chamber dilatation and signs of pulmonary hypertension were noted. The patient subsequently underwent surgical repair, and intraoperative findings correlated with CT imaging.
Conclusion: ECG-gated CT angiography provides precise localization of the rupture site, delineation of the fistulous tract, and assessment of valvular involvement, thereby playing a crucial role in preoperative planning of ruptured sinus of Valsalva aneurysms.
Keywords:Ruptured Sinus of Valsalva aneurysm; ECG-gated CT; CT angiography; Aortic root; Pulmonary hypertension
Introduction
Sinus of Valsalva aneurysm (SOVA) is a rare cardiac abnormality
that may be congenital or acquired. These aneurysms arise due to
weakness at the junction between the aortic media and the annulus
fibrosus. Although many remain asymptomatic, rupture of the
aneurysm can result in an acute left-to-right shunt, leading to
congestive cardiac failure, pulmonary hypertension, or cardiogenic
shock [1-3].
The right coronary sinus is most commonly involved, followed by the non-coronary sinus [1,3]. Rupture into right-sided cardiac chambers is the typical pattern [2,4].
Transthoracic echocardiography is frequently used as a screening tool; however, CT angiography provides superior spatial resolution and allows accurate delineation of the rupture site, fistulous tract, and associated structural abnormalities. This detailed anatomical information is essential for surgical planning [4,5].
We report a case of a ruptured non-coronary sinus of Valsalva aneurysm draining into the right atrium, initially diagnosed on ECGgated CT angiography and confirmed at surgery.
The right coronary sinus is most commonly involved, followed by the non-coronary sinus [1,3]. Rupture into right-sided cardiac chambers is the typical pattern [2,4].
Transthoracic echocardiography is frequently used as a screening tool; however, CT angiography provides superior spatial resolution and allows accurate delineation of the rupture site, fistulous tract, and associated structural abnormalities. This detailed anatomical information is essential for surgical planning [4,5].
We report a case of a ruptured non-coronary sinus of Valsalva aneurysm draining into the right atrium, initially diagnosed on ECGgated CT angiography and confirmed at surgery.
Case Report
A 41-year-old female with no known comorbidities presented
with progressive shortness of breath over a period of two months,
which had worsened significantly over the preceding two to three
weeks. She also reported orthopnea, palpitations, intermittent chest
discomfort, nausea, vomiting, bilateral lower limb edema, and
episodes of hypotension.
She was initially treated elsewhere for unstable angina with acute left ventricular failure and cardiogenic shock and received inotropic and vasodilator support. Despite initial improvement, she developed recurrent dyspnea and was found to have pulmonary hypertension, ascites, and anemia during further evaluation.
On admission, her pulse rate was 78 beats per minute, blood pressure was 186/68 mmHg, respiratory rate was 24 breaths per minute, and oxygen saturation was 97% on room air. Cardiac auscultation revealed a pansystolic murmur.
Coronary angiography was performed via the right femoral approach and demonstrated normal coronary arteries. In view of persistent symptoms and suspected structural cardiac pathology, the patient was referred for CT aortography.
She was initially treated elsewhere for unstable angina with acute left ventricular failure and cardiogenic shock and received inotropic and vasodilator support. Despite initial improvement, she developed recurrent dyspnea and was found to have pulmonary hypertension, ascites, and anemia during further evaluation.
On admission, her pulse rate was 78 beats per minute, blood pressure was 186/68 mmHg, respiratory rate was 24 breaths per minute, and oxygen saturation was 97% on room air. Cardiac auscultation revealed a pansystolic murmur.
Coronary angiography was performed via the right femoral approach and demonstrated normal coronary arteries. In view of persistent symptoms and suspected structural cardiac pathology, the patient was referred for CT aortography.
CT Technique:
ECG-gated contrast-enhanced CT aortography was performed
on a dual-source dual-energy 128-slice CT scanner (Siemens
Somatom Drive). A retrospective ECG-gated acquisition was used.
Intravenous administration of 100 mL of non-ionic iodinated contrast
was performed, followed by thin-section image reconstruction.
Multiplanar reformations, maximum intensity projections, and
volume-rendered images were generated for detailed anatomical
assessment.Imaging Findings:
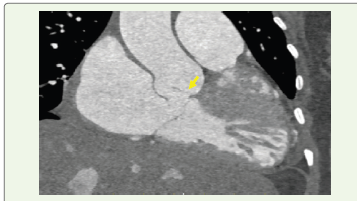
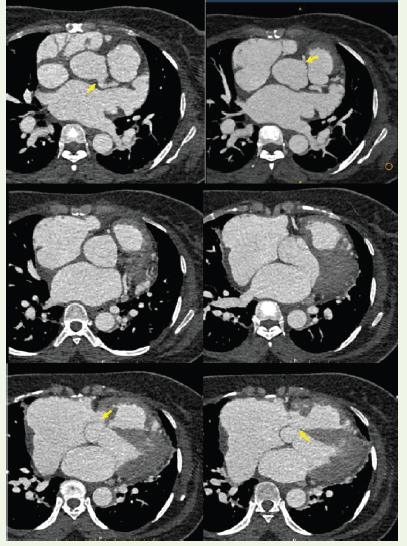
CT angiography demonstrated a focal aneurysmal dilatation
arising from the non-coronary sinus of Valsalva, measuring
approximately 18 × 14 mm. A well-defined rupture defect measuring
approximately 12.5 × 11.4 mm was identified in the wall of the
aneurysmal sac. Through this defect, contrast was seen directly
opacifying the right atrium, confirming the presence of a fistulous
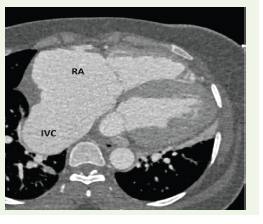
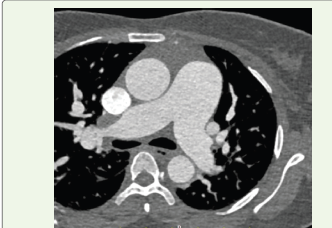
communication.The aneurysmal sac was noted to protrude into the right atrium, producing indentation of the adjacent tricuspid valve leaflet. There was significant dilatation of the right atrium and inferior vena cava, with associated hepatic venous congestion. The main pulmonary artery was dilated, measuring approximately 3.9 cm, suggestive of pulmonary hypertension. Mild pericardial effusion and cardiomegaly were also present.
The right and left coronary sinuses were unremarkable. The coronary arteries, thoracic aorta, and abdominal aorta were within normal limits.
Surgical Correlation:
The patient subsequently underwent surgical repair. Intraoperative
findings confirmed a ruptured sinus of Valsalva aneurysm opening
into the right atrium. The aneurysmal sac was identified and excised.
The sinus defect was repaired using a Dacron patch, and tricuspid
valve repair was also performed. The postoperative course was
uneventful, and the patient remained hemodynamically stable.Postoperative Course and Follow-Up:
The patient was shifted to the intensive care unit following surgery
and remained hemodynamically stable. Inotropic support was
gradually tapered, and she was extubated on the second postoperative
day. Postoperative echocardiography demonstrated satisfactory
repair with no residual shunt across the sinus defect and preserved left
ventricular systolic function (LVEF approximately 55%). The patient
had an uneventful recovery and was discharged in stable condition
with advice for routine cardiothoracic follow-up.Discussion
Sinus of Valsalva aneurysm (SOVA) is an uncommon abnormality
of the aortic root characterized by focal dilatation of one of the aortic
sinuses. The condition most frequently results from congenital
deficiency of elastic and muscular tissue at the junction between
the aortic media and annulus fibrosus [1,3]. Acquired causes such
as infective endocarditis, trauma, or degenerative changes are less
common but have also been described [5,6]. Progressive weakening
of the sinus wall may eventually culminate in rupture, producing
a pathological communication between the aorta and an adjacent
cardiac chamber.
The right coronary sinus is most commonly involved, followed by the non-coronary sinus, while left sinus involvement is rare [1,3]. Patterns of rupture reflect anatomical proximity. The right coronary sinus most often ruptures into the right ventricle, whereas aneurysms arising from the non-coronary sinus typically communicate with the right atrium [1,2,4]. Our case demonstrated a ruptured non-coronary sinus aneurysm draining into the right atrium, which corresponds to the recognized distribution patterns reported in the literature.
Clinical manifestations depend on the size of the defect and the rapidity of shunt formation. Small unruptured aneurysms may remain asymptomatic, whereas rupture commonly produces an acute left-to-right shunt leading to dyspnea, volume overload, and signs of heart failure [2,7]. Chronic shunting may result in progressive right atrial enlargement, pulmonary hypertension, and secondary valvular dysfunction. In the present patient, right atrial dilatation, inferior
The right coronary sinus is most commonly involved, followed by the non-coronary sinus, while left sinus involvement is rare [1,3]. Patterns of rupture reflect anatomical proximity. The right coronary sinus most often ruptures into the right ventricle, whereas aneurysms arising from the non-coronary sinus typically communicate with the right atrium [1,2,4]. Our case demonstrated a ruptured non-coronary sinus aneurysm draining into the right atrium, which corresponds to the recognized distribution patterns reported in the literature.
Clinical manifestations depend on the size of the defect and the rapidity of shunt formation. Small unruptured aneurysms may remain asymptomatic, whereas rupture commonly produces an acute left-to-right shunt leading to dyspnea, volume overload, and signs of heart failure [2,7]. Chronic shunting may result in progressive right atrial enlargement, pulmonary hypertension, and secondary valvular dysfunction. In the present patient, right atrial dilatation, inferior
vena cava enlargement, and pulmonary arterial dilatation were
evident on CT, reflecting significant hemodynamic impact.
Imaging is central to diagnosis and therapeutic planning.
Transthoracic echocardiography is often the first-line investigation
because it can demonstrate abnormal flow jets and chamber
enlargement. However, acoustic window limitations and complex
anatomy may hinder precise localization of the rupture site [4,5].
Cross-sectional imaging provides a more comprehensive anatomical
assessment.
Multidetector CT angiography, particularly when ECGgated, enables high spatial resolution evaluation of the aortic root, aneurysmal sac, and fistulous tract [4,8,10]. ECG gating minimizes motion artifact and allows accurate delineation of the aortic root and coronary origins, which is crucial in preoperative planning.
Cross-sectional imaging not only defines the rupture site but also assesses coronary ostial involvement, chamber enlargement, pulmonary arterial changes, and associated congenital anomalies [11]. Such evaluation is essential because coronary compromise or concomitant structural abnormalities may alter surgical strategy. In our case, CT clearly demonstrated a focal rupture defect within the non-coronary sinus, direct opacification of the right atrium, indentation of the tricuspid valve leaflet, and preserved coronary ostia. The ability to visualize these relationships in multiple planes provided a precise anatomical roadmap prior to surgery.
Complications of SOVA include aortic regurgitation, arrhythmias, endocarditis, progressive pulmonary hypertension, and, in severe cases, cardiogenic shock [2,5]. Long-term surgical outcomes are generally favorable when timely repair is performed [2,7]. Accurate preoperative anatomical definition has been shown to contribute to optimal surgical results [4,5].
This case underscores the diagnostic strength of ECG-gated CT angiography in ruptured SOVA. While echocardiography remains indispensable for functional assessment, CT offers superior depiction of the rupture tract, spatial relationships, and associated structural changes. Such detailed anatomical information is particularly valuable when surgical repair is contemplated.
Multidetector CT angiography, particularly when ECGgated, enables high spatial resolution evaluation of the aortic root, aneurysmal sac, and fistulous tract [4,8,10]. ECG gating minimizes motion artifact and allows accurate delineation of the aortic root and coronary origins, which is crucial in preoperative planning.
Cross-sectional imaging not only defines the rupture site but also assesses coronary ostial involvement, chamber enlargement, pulmonary arterial changes, and associated congenital anomalies [11]. Such evaluation is essential because coronary compromise or concomitant structural abnormalities may alter surgical strategy. In our case, CT clearly demonstrated a focal rupture defect within the non-coronary sinus, direct opacification of the right atrium, indentation of the tricuspid valve leaflet, and preserved coronary ostia. The ability to visualize these relationships in multiple planes provided a precise anatomical roadmap prior to surgery.
Complications of SOVA include aortic regurgitation, arrhythmias, endocarditis, progressive pulmonary hypertension, and, in severe cases, cardiogenic shock [2,5]. Long-term surgical outcomes are generally favorable when timely repair is performed [2,7]. Accurate preoperative anatomical definition has been shown to contribute to optimal surgical results [4,5].
This case underscores the diagnostic strength of ECG-gated CT angiography in ruptured SOVA. While echocardiography remains indispensable for functional assessment, CT offers superior depiction of the rupture tract, spatial relationships, and associated structural changes. Such detailed anatomical information is particularly valuable when surgical repair is contemplated.
Conclusion
ECG-gated dual-source CT angiography plays a crucial role in
the evaluation of ruptured sinus of Valsalva aneurysms by precisely
delineating the rupture site, fistulous communication, and associated
valvular involvement, thereby facilitating optimal surgical planning.
This detailed anatomical information is invaluable for preoperative
planning and surgical decision-making.
Acknowledgements
The authors would like to thank the Department of Cardiothoracic
Surgery at Jaslok Hospital and Research Centre for their valuable
surgical input and intraoperative correlation in this case.
References
Citation
Ajith V, Karnavat C, Desai SB. ECG-Gated High Resolution CT Evaluation of a Ruptured Non-Coronary Sinus of Valsalva Aneurysm Draining into the Right Atrium: A Case Report. Indian J Appl Radiol. 2026;12(1): 230.