Research Article
Quantitative CT Markers for Early Prediction of Severity in Acute Pancreatitis A Prospective Observational Study
Janakare AH*, Kulkarni AM, Indushree TV and Parthasarathy KR
Department of Radiodiagnosis SS Institute of Medical Sciences and Research Centre Davangere, Karnataka, India
*Corresponding author:Dr. Akshay H. Janakare, Department of Radiodiagnosis SS Institute of Medical Sciences and Research Centre Davangere, Karnataka, India. E-mail Id: akshayjanakare@gmail.com
Copyright: © 2026 Janakare AH, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information: Submission: 12/02/2026; Accepted: 08/04/2026; Published: 10/04/2026
Abstract
Objective: To evaluate quantitative CT markers in acute pancreatitis and identify the strongest predictor of severe disease and adverse outcomes.
Materials and Methods: This prospective observational study included 50 patients with clinically and biochemically confirmed acute pancreatitis who underwent contrast-enhanced CT (CECT) within 5–7 days after symptom onset (mean: 5 + 2 days). Quantitative parameters assessed were percentage pancreatic necrosis, extrapancreatic necrosis (EN) volume, peripancreatic fluid volume using 3D volumetry, and peripancreatic fat attenuation. Findings were correlated with the Revised Atlanta Classification and clinical outcomes.
Results: Severe acute pancreatitis was observed in 24% of patients. Extrapancreatic necrosis volume demonstrated the highest diagnostic accuracy for severe disease (area under the ROC curve [AUC] 0.89; cutoff >120 mL), outperforming pancreatic necrosis percentage and other quantitative markers..
Conclusion: Extrapancreatic necrosis volume is the most reliable quantitative CT marker for predicting severe acute pancreatitis and adverse clinical outcomes.
Materials and Methods: This prospective observational study included 50 patients with clinically and biochemically confirmed acute pancreatitis who underwent contrast-enhanced CT (CECT) within 5–7 days after symptom onset (mean: 5 + 2 days). Quantitative parameters assessed were percentage pancreatic necrosis, extrapancreatic necrosis (EN) volume, peripancreatic fluid volume using 3D volumetry, and peripancreatic fat attenuation. Findings were correlated with the Revised Atlanta Classification and clinical outcomes.
Results: Severe acute pancreatitis was observed in 24% of patients. Extrapancreatic necrosis volume demonstrated the highest diagnostic accuracy for severe disease (area under the ROC curve [AUC] 0.89; cutoff >120 mL), outperforming pancreatic necrosis percentage and other quantitative markers..
Conclusion: Extrapancreatic necrosis volume is the most reliable quantitative CT marker for predicting severe acute pancreatitis and adverse clinical outcomes.
Keywords:Acute pancreatitis; Quantitative CT; Extrapancreatic necrosis; Severity prediction
Introduction
Acute pancreatitis is a common and potentially life-threatening
abdominal emergency with a clinical spectrum ranging from mild
self-limiting inflammation to severe necrotizing disease associated
with multiorgan failure and high mortality [1,3] Early identification
of patients at risk for severe disease is critical for optimizing clinical
management, guiding intensive care unit (ICU) admission, and
improving outcomes [1,4,7].
Conventional clinical scoring systems such as Ranson’s criteria, BISAP, and APACHE II are widely used for prognostication; however, they require serial assessments and incorporate subjective or delayed parameters, limiting their utility in early decision-making. Imaging, particularly contrast-enhanced computed tomography (CECT), plays a pivotal role not only in confirming diagnosis but also in assessing disease severity, detecting complications, and guiding therapeutic interventions [1,6,7].
Traditional CT-based indices such as the CT Severity Index (CTSI) and Modified CTSI rely on semi-quantitative or categorical assessment of pancreatic inflammation and necrosis. However, these approaches may lack precision and reproducibility [6,7]. In recent years, there has been growing interest in quantitative imaging biomarkers that provide objective and reproducible metrics of disease burden.
Conventional clinical scoring systems such as Ranson’s criteria, BISAP, and APACHE II are widely used for prognostication; however, they require serial assessments and incorporate subjective or delayed parameters, limiting their utility in early decision-making. Imaging, particularly contrast-enhanced computed tomography (CECT), plays a pivotal role not only in confirming diagnosis but also in assessing disease severity, detecting complications, and guiding therapeutic interventions [1,6,7].
Traditional CT-based indices such as the CT Severity Index (CTSI) and Modified CTSI rely on semi-quantitative or categorical assessment of pancreatic inflammation and necrosis. However, these approaches may lack precision and reproducibility [6,7]. In recent years, there has been growing interest in quantitative imaging biomarkers that provide objective and reproducible metrics of disease burden.
Extrapancreatic necrosis (EN), representing the extent of
inflammatory spread beyond the pancreas, has emerged as a potential
key determinant of disease severity [8,12]. Quantitative volumetric
assessment of EN and associated inflammatory changes may offer
superior predictive value compared to conventional parameters.
This study aims to evaluate quantitative CT markers in acute pancreatitis and identify the most reliable imaging predictor of severe disease and adverse clinical outcomes, thereby enhancing early risk stratification and clinical decision-making.
This study aims to evaluate quantitative CT markers in acute pancreatitis and identify the most reliable imaging predictor of severe disease and adverse clinical outcomes, thereby enhancing early risk stratification and clinical decision-making.
Materials and Methods
Ethics Statement:
The study was approved by the Institutional Ethics Committee.
Written informed consent was obtained from all participants prior to
inclusion in the study. All procedures were conducted in accordance
with the ethical standards of the institutional research committee and
with the Declaration of Helsinki. Patient confidentiality was strictly
maintained, and all imaging and clinical data were anonymized.Study Design:
Prospective observational study.Study Population:
Fifty consecutive patients with acute pancreatitis were included.Inclusion Criteria:
Clinically and biochemically confirmed acute pancreatitis
CECT performed within 5-7 days of symptom onsetExclusion Criteria:
Chronic pancreatitis
Prior pancreatic surgery
Poor-quality CT imagesCT Protocol:
CECT was performed on a 128-slice multidetector CT scanner
using a triphasic acquisition protocol. All contrast-enhanced CT
scans were performed between 5–7 days after symptom onset,
corresponding to the early necrotizing phase of acute pancreatitis.This timing was standardized to optimize detection of pancreatic and extrapancreatic necrosis.
Quantitative Parameters Assessed
Percentage pancreatic necrosis
Extrapancreatic necrosis (EN) volume
Peripancreatic fluid collection volume
Peripancreatic fat attenuation (in Hounsfield units)
Statistical Analysis:
Logistic regression and receiver operating characteristic (ROC)
curve analysis were performed. The area under the ROC curve (AUC)
was calculated to assess diagnostic performance. An AUC closer to
1.0 indicated excellent predictive accuracy, whereas a value of 0.5
indicated no discriminatory ability.A p-value < 0.05 was considered statistically significant. Optimal
cutoff values were determined using the Youden Index (J = Sensitivity
+ Specificity – 1), selecting the threshold that maximized combined
sensitivity and specificity for predicting severe acute pancreatitis.
Severity grading was performed according to the Revised Atlanta
Classification (2012) [3], integrating clinical parameters such as
organ failure with imaging findings including pancreatic necrosis,
extrapancreatic necrosis, and peripancreatic collections.
Results
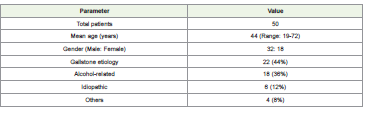
A total of 50 patients were included. The mean age was 44 years
(range: 19–72 years), with male predominance (32 males, 18 females).
Gallstone disease was the most common etiology (44%), followed by
alcohol-related pancreatitis (36%). Other causes included idiopathic
and miscellaneous etiologies [Table 1] .
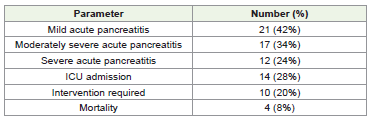
Based on the Revised Atlanta Classification, [3] 21 patients (42%) had mild acute pancreatitis, 17 (34%) had moderately severe disease, and 12 (24%) had severe acute pancreatitis. ICU admission was required in 14 patients (28%), interventional procedures were performed in 10 patients (20%), and 4 patients (8%) died [Table 2].
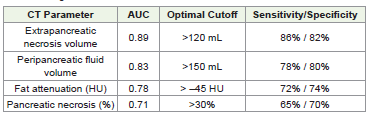
Quantitative CT analysis demonstrated that extrapancreatic necrosis volume was significantly higher in patients with severe disease. ROC analysis showed that EN volume had the highest diagnostic accuracy (AUC 0.89) at an optimal cutoff value of >120 mL, yielding 86% sensitivity and 82% specificity.
Peripancreatic fluid volume demonstrated good performance (AUC 0.83) at a cutoff >150 mL. Increased peripancreatic fat attenuation showed moderate predictive value (AUC 0.78; cutoff > –45 HU), while percentage pancreatic necrosis demonstrated lower accuracy (AUC 0.71; cutoff >30%).
An EN volume greater than 120 mL was strongly associated with severe acute pancreatitis. Similarly, peripancreatic fluid volume exceeding 150 mL and pancreatic necrosis greater than 30% were more frequently observed in severe cases. The diagnostic performance of all quantitative CT markers is summarized in [Table 3].
Based on the Revised Atlanta Classification, [3] 21 patients (42%) had mild acute pancreatitis, 17 (34%) had moderately severe disease, and 12 (24%) had severe acute pancreatitis. ICU admission was required in 14 patients (28%), interventional procedures were performed in 10 patients (20%), and 4 patients (8%) died [Table 2].
Quantitative CT analysis demonstrated that extrapancreatic necrosis volume was significantly higher in patients with severe disease. ROC analysis showed that EN volume had the highest diagnostic accuracy (AUC 0.89) at an optimal cutoff value of >120 mL, yielding 86% sensitivity and 82% specificity.
Peripancreatic fluid volume demonstrated good performance (AUC 0.83) at a cutoff >150 mL. Increased peripancreatic fat attenuation showed moderate predictive value (AUC 0.78; cutoff > –45 HU), while percentage pancreatic necrosis demonstrated lower accuracy (AUC 0.71; cutoff >30%).
An EN volume greater than 120 mL was strongly associated with severe acute pancreatitis. Similarly, peripancreatic fluid volume exceeding 150 mL and pancreatic necrosis greater than 30% were more frequently observed in severe cases. The diagnostic performance of all quantitative CT markers is summarized in [Table 3].
Patients with severe acute pancreatitis more frequently
demonstrated extensive extrapancreatic necrosis, larger peripancreatic
collections, and higher attenuation of surrounding fat, reflecting a
more intense inflammatory response. These patients required more
aggressive management, including ICU admission and interventional
procedures such as percutaneous drainage. Mortality was observed
exclusively in the severe group, underscoring the importance of early
imaging-based risk stratification.
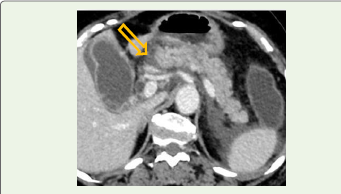
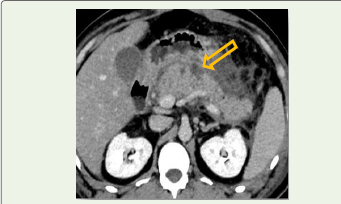
Representative Case Illustration:
A 48-year-old male with a history of chronic alcohol use presented
with acute onset severe epigastric pain radiating to the back, associated
with vomiting. Laboratory evaluation revealed significantly elevated
serum amylase and lipase levels.Contrast-enhanced CT performed on day 5 of symptom onset demonstrated extensive areas of non-enhancing pancreatic parenchyma involving more than 60% of the gland, along with largevolume extrapancreatic necrosis extending into the anterior pararenal space and mesenteric root [Figure 3].
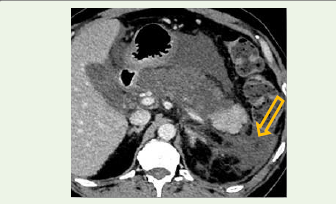
Quantitative volumetric analysis revealed extrapancreatic necrosis volume exceeding 150 mL and significant peripancreatic fluid collections [Figure 4].
The patient developed persistent organ failure requiring ICU admission and underwent percutaneous drainage for necrotic collections. The clinical course was complicated by prolonged hospitalization; however, the patient showed gradual recovery with multidisciplinary management.
This case highlights the strong correlation between increased extrapancreatic necrosis volume and severe disease, emphasizing its role as a reliable imaging biomarker for predicting adverse outcomes.

Discussion
Early prediction of disease severity in acute pancreatitis remains
a major clinical challenge. Severe acute pancreatitis is associated with
significant morbidity, prolonged hospitalization, increased need for
interventions, and higher mortality [13,14]. Therefore, reliable early
imaging biomarkers are essential for risk stratification and guiding
management.
In the present study, extrapancreatic necrosis (EN) volume demonstrated the highest diagnostic accuracy for predicting severe disease (AUC 0.89), outperforming traditional parameters such as percentage pancreatic necrosis and peripancreatic fat attenuation. These findings are consistent with emerging literature emphasizing the prognostic importance of extrapancreatic inflammatory burden [8,12].
Previous studies have highlighted that pancreatic necrosis alone may not fully reflect disease severity, as patients with limited parenchymal necrosis can still develop severe systemic complications due to widespread inflammatory response. EN represents the extent of inflammation extending into peripancreatic and retroperitoneal spaces, which plays a crucial role in triggering systemic inflammatory response syndrome (SIRS) [8] and organ failure.
Compared to conventional scoring systems such as CTSI and Modified CTSI [6,7] which rely on categorical grading, quantitative volumetric assessment provides continuous, objective data. This reduces interobserver variability and improves reproducibility¹³, making it more suitable for standardized reporting. Our study adds to the growing body of evidence by demonstrating a clear cutoff value (>120 mL) for EN volume with high sensitivity and specificity for predicting severe disease. This quantitative threshold may serve as a practical imaging biomarker in routine clinical practice.
In the present study, extrapancreatic necrosis (EN) volume demonstrated the highest diagnostic accuracy for predicting severe disease (AUC 0.89), outperforming traditional parameters such as percentage pancreatic necrosis and peripancreatic fat attenuation. These findings are consistent with emerging literature emphasizing the prognostic importance of extrapancreatic inflammatory burden [8,12].
Previous studies have highlighted that pancreatic necrosis alone may not fully reflect disease severity, as patients with limited parenchymal necrosis can still develop severe systemic complications due to widespread inflammatory response. EN represents the extent of inflammation extending into peripancreatic and retroperitoneal spaces, which plays a crucial role in triggering systemic inflammatory response syndrome (SIRS) [8] and organ failure.
Compared to conventional scoring systems such as CTSI and Modified CTSI [6,7] which rely on categorical grading, quantitative volumetric assessment provides continuous, objective data. This reduces interobserver variability and improves reproducibility¹³, making it more suitable for standardized reporting. Our study adds to the growing body of evidence by demonstrating a clear cutoff value (>120 mL) for EN volume with high sensitivity and specificity for predicting severe disease. This quantitative threshold may serve as a practical imaging biomarker in routine clinical practice.
Clinical Implications
The incorporation of quantitative EN volume assessment into
routine CT reporting can significantly impact patient management.
Patients identified as high-risk based on EN volume may benefit from
early ICU admission, aggressive monitoring, timely intervention, and
multidisciplinary care.
Contribution to Current Knowledge:
This study reinforces that extrapancreatic inflammatory burden
is a stronger predictor of severity than pancreatic necrosis alone and
supports integration of quantitative imaging biomarkers into future
severity scoring systems.Despite its promising findings, further multicentric studies with larger sample sizes are required for validation.
Conclusion
Quantitative volumetric assessment of extrapancreatic necrosis
provides superior predictive accuracy compared to traditional CT
severity indices. Integration of this objective marker with established
clinical and radiological classification systems may enhance early risk
stratification and improve patient management.
Future integration of artificial intelligence–based automated volumetric analysis may further enhance the accuracy and clinical applicability of quantitative CT biomarkers.
Future integration of artificial intelligence–based automated volumetric analysis may further enhance the accuracy and clinical applicability of quantitative CT biomarkers.
Limitations:
This study was limited by its single-center design and relatively
small sample size. Quantitative measurements required manual
segmentation, which may introduce observer variability. Lack
of longitudinal follow-up imaging and correlation with serial
biochemical inflammatory markers were additional limitations.References
Citation
Janakare AH, Kulkarni AM, Indushree TV, Parthasarathy KR. Quantitative CT Markers for Early Prediction of Severity in Acute Pancreatitis: A Prospective Observational Study. Indian J Appl Radiol. 2026;12(1): 229.