Case Report
Orbital Encephalocele Due to Sphenoid Wing Dysplasia in Neurofibromatosis Type 1: A Case Report Highlighting a Diagnostic Pitfall
Nikita Mary Baby*
Consultant Radiologist, Government Medical College, Ernakulam, Kerala, India
*Corresponding author:Dr. Nikita Mary Baby, Consultant Radiologist Department of Radiodiagnosis, Government Medical College, Ernakulam, Kerala, India, Email: nikita92.nmb@gmail.com
Copyright: © 2026 Baby NM. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information:Submission: 26/12/2025; Accepted: 05/02/2026; Published: 07/02/2026
Abstract
Neurofibromatosis type 1 (NF-1) is a multisystem genetic disorder characterized by cutaneous, neurological, and skeletal manifestations. Sphenoid wing dysplasia is a characteristic but relatively uncommon osseous abnormality in NF-1 and may result in herniation of intracranial contents into the orbit, producing an orbital encephalocele and progressive proptosis. In routine clinical practice, imaging evaluation of proptosis in NF-1 often prioritizes exclusion of optic pathway glioma or optic nerve sheath meningioma, which may lead to under-recognition of sphenoid wing dysplasia and its complications.
Consequently, orbital encephalocele may be misdiagnosed as an arachnoid cyst.
This report describes two patients with NF-1—one pediatric and one adult—both presenting with unilateral proptosis and previously misdiagnosed as having arachnoid cysts. Through these cases, characteristic CT and MRI features facilitating accurate diagnosis are highlighted, emphasizing the importance of careful skull base assessment to avoid this important diagnostic pitfall.
Consequently, orbital encephalocele may be misdiagnosed as an arachnoid cyst.
This report describes two patients with NF-1—one pediatric and one adult—both presenting with unilateral proptosis and previously misdiagnosed as having arachnoid cysts. Through these cases, characteristic CT and MRI features facilitating accurate diagnosis are highlighted, emphasizing the importance of careful skull base assessment to avoid this important diagnostic pitfall.
Keywords: Neurofibromatosis type 1; Sphenoid wing dysplasia; Orbital encephalocele; Proptosis; Arachnoid cyst; Diagnostic pitfall
Neurofibromatosis type 1 (NF-1) is a common autosomal
dominant neurocutaneous disorder caused by pathogenic variants
in the NF1 gene on chromosome 17, with an estimated incidence of
approximately 1 in 3,000 individuals. The disease is characterized
by marked phenotypic heterogeneity and involves multiple organ
systems, including the skin, nervous system, and skeleton. While
cutaneous manifestations and optic pathway gliomas are well
recognized and frequently emphasized in clinical practice, skeletal
abnormalities—despite being part of the diagnostic criteria—are
comparatively under-recognized.
Sphenoid wing dysplasia is a characteristic but relatively
uncommon skeletal manifestation of NF-1, reported in approximately
5–10% of affected individuals. Partial or complete absence of the
sphenoid wing results in loss of the normal osseous barrier between
the orbit and the middle cranial fossa, predisposing to herniation of
cerebrospinal fluid (CSF) and brain parenchyma into the orbit. This
may lead to the development of an orbital encephalocele, presenting
clinically with progressive, often unilateral proptosis and potential
optic nerve compression.
In routine imaging evaluation of proptosis in patients with NFNeurofibromatosis
1, diagnostic attention is frequently directed toward excluding optic
pathway glioma or optic nerve sheath meningioma, given their
strong association with the disease. This diagnostic bias may result in
under-recognition of sphenoid wing dysplasia and its complications.
Furthermore, because orbital encephaloceles often demonstrate
CSF-like signal characteristics on MRI, they may be misdiagnosed as
arachnoid cysts, particularly when osseous abnormalities are subtle
or not adequately assessed.
This case series describes two patients with NF-1—one adult and
one pediatric—both presenting with unilateral proptosis and initially
misdiagnosed as having arachnoid cysts. Through detailed CT–MRI
correlation, this report highlights characteristic imaging features that
facilitate accurate diagnosis, underscores an important diagnostic
pitfall, and emphasizes the clinical and management implications of
early recognition.
Ethical Considerations:
Written informed consent was obtained from both patients
and/or their legal guardians for publication of clinical details and
imaging findings. All procedures were conducted in accordance with
institutional ethical standards and the principles of the Declaration
of Helsinki.Case Series:
Case 1A 39-year-old man with a known diagnosis of neurofibromatosis type 1 presented with progressively increasing left-sided proptosis over several years. The patient reported mild visual discomfort but no acute visual loss, diplopia, or pain. There was no history of trauma or prior orbital surgery. Clinical examination revealed non-pulsatile left proptosis without signs of acute inflammation.
MRI of the brain and orbits with contrast demonstrated hypoplasia of the left sphenoid wing with herniation of brain parenchyma and CSF into the superior aspect of the left orbit, consistent with a left
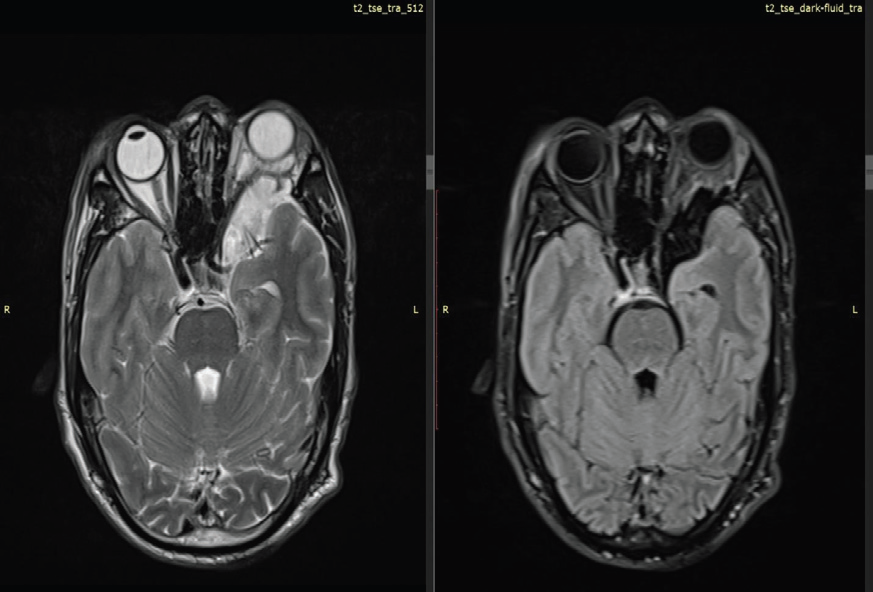
orbital encephalocele. This resulted in left-sided proptosis with
compression and mild medial deviation of the intraorbital segment
of the left optic nerve. Marked narrowing of the left superior orbital
fissure was noted, with optic nerve compression at this level.
Prominent arachnoid spaces were seen in the left anterior temporal region secondary to the encephalocele, with medial displacement of the left middle cerebral artery. No abnormal enlargement or postcontrast enhancement of the optic nerve was identified, effectively excluding optic nerve glioma and optic nerve sheath meningioma. Additional findings included multiple scalp neurofibromas and T2/FLAIR hyperintense foci involving the bilateral thalami and periventricular regions, consistent with focal areas of signal intensity (FASI). The left sphenoid sinus was hypoplastic.
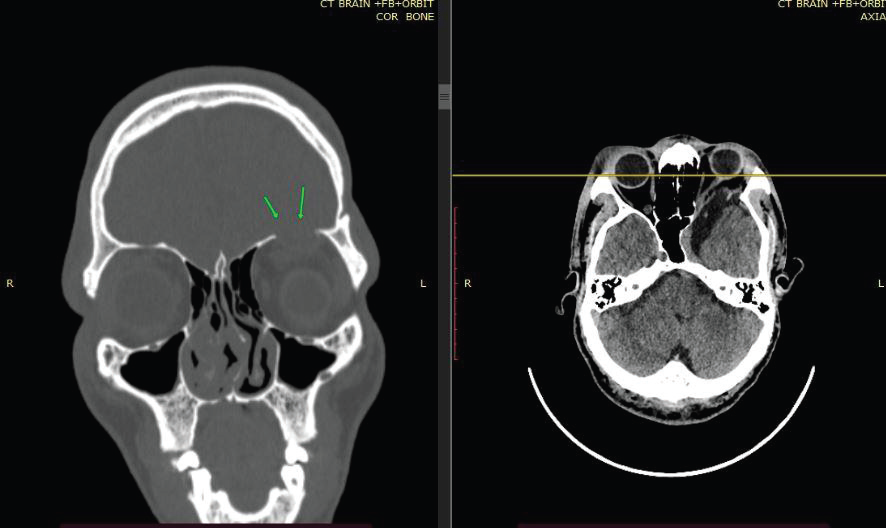
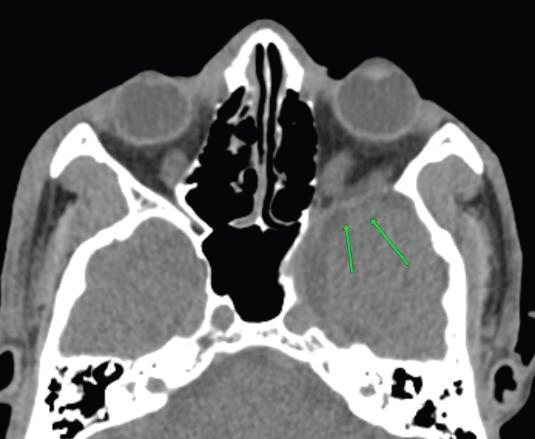
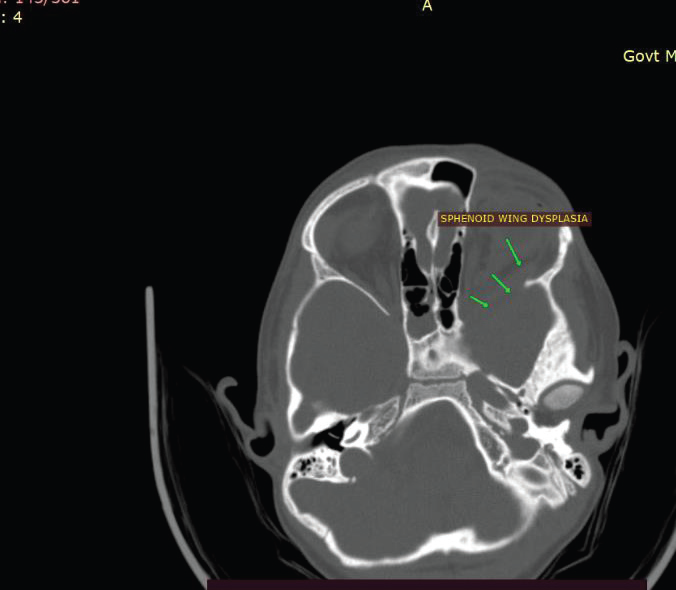
CT of the skull base confirmed hypoplasia of the left sphenoid wing with loss of the normal bony separation between the middle cranial fossa and the orbit. Prior imaging studies had described the lesion as an arachnoid cyst, leading to delayed recognition of the underlying pathology.
The patient was referred for multidisciplinary evaluation, and given the slowly progressive nature of symptoms and preserved vision, conservative management with clinical and imaging followup was advised.
Prominent arachnoid spaces were seen in the left anterior temporal region secondary to the encephalocele, with medial displacement of the left middle cerebral artery. No abnormal enlargement or postcontrast enhancement of the optic nerve was identified, effectively excluding optic nerve glioma and optic nerve sheath meningioma. Additional findings included multiple scalp neurofibromas and T2/FLAIR hyperintense foci involving the bilateral thalami and periventricular regions, consistent with focal areas of signal intensity (FASI). The left sphenoid sinus was hypoplastic.
CT of the skull base confirmed hypoplasia of the left sphenoid wing with loss of the normal bony separation between the middle cranial fossa and the orbit. Prior imaging studies had described the lesion as an arachnoid cyst, leading to delayed recognition of the underlying pathology.
The patient was referred for multidisciplinary evaluation, and given the slowly progressive nature of symptoms and preserved vision, conservative management with clinical and imaging followup was advised.
Case 2:
An 8-year-old boy, born to a mother with neurofibromatosis type
1, presented with gradually progressive left-sided proptosis noted by
caregivers over the preceding year. There was no history of trauma,
pain, or visual complaints. Ophthalmologic evaluation revealed mild
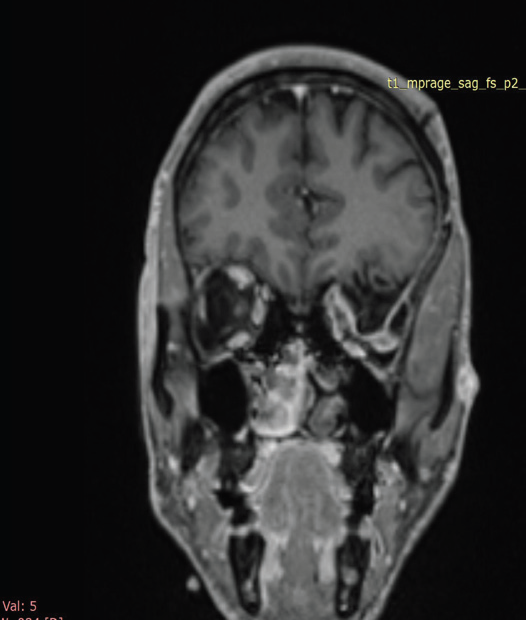
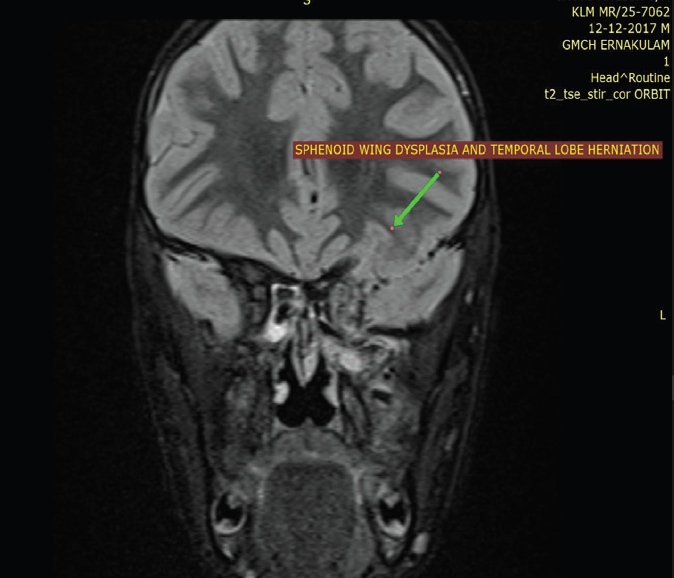
asymmetry of the globes without acute visual deficit.MRI of the brain and orbits with contrast, supplemented by CT imaging, revealed dysplasia of the left sphenoid wing with anterior herniation of the left temporal lobe into the posterior aspect of the left orbit, consistent with an orbital encephalocele. This resulted in leftsided proptosis and mild asymmetric enlargement of the left globe.
The left medial and lateral rectus muscles were enlarged and demonstrated post-contrast enhancement, suggestive of extraocular
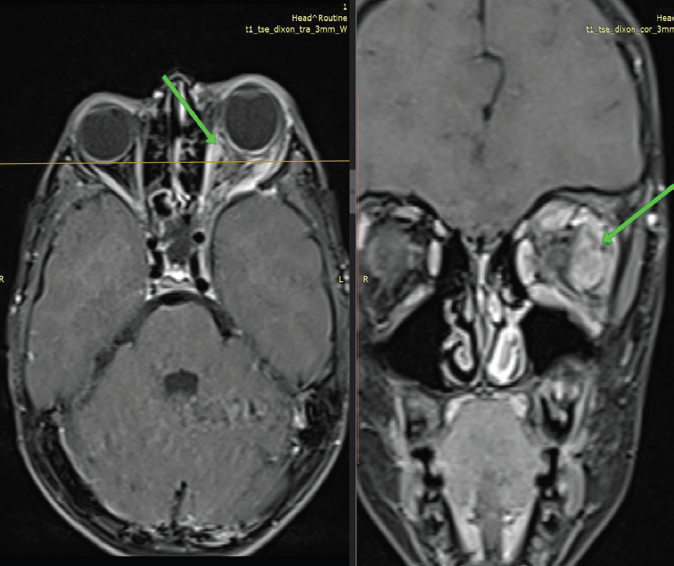
muscle neurofibromas, with mild surrounding orbital fat stranding.
The intraorbital segment of the left optic nerve appeared mildly
tortuous but showed no enlargement or abnormal enhancement.
CT demonstrated absence of tram-track calcification, excluding
optic nerve sheath meningioma. The left superior orbital fissure was
asymmetrically enlarged, and the left sphenoid sinus was hypoplastic.
MRI of the brain demonstrated multiple non-enhancing T2/ FLAIR hyperintense lesions involving the bilateral globus pallidi, thalami, cerebellum, and cerebral peduncles, characteristic of FASI. No diffusion restriction or mass effect was observed. As in the first case, the lesion had previously been interpreted as an arachnoid cyst.
Given the patient’s age and absence of visual compromise, a conservative approach with close ophthalmologic and radiologic surveillance was recommended.
MRI of the brain demonstrated multiple non-enhancing T2/ FLAIR hyperintense lesions involving the bilateral globus pallidi, thalami, cerebellum, and cerebral peduncles, characteristic of FASI. No diffusion restriction or mass effect was observed. As in the first case, the lesion had previously been interpreted as an arachnoid cyst.
Given the patient’s age and absence of visual compromise, a conservative approach with close ophthalmologic and radiologic surveillance was recommended.
Discussion
Sphenoid wing dysplasia is a distinctive skeletal manifestation
of neurofibromatosis type 1 and represents an important cause of
unilateral proptosis in this population. Although included in the
diagnostic criteria for NF-1, it remains relatively uncommon and
is therefore frequently overlooked in routine imaging practice. The
underlying pathogenesis is not fully understood but is thought to
involve abnormal mesodermal development, progressive osseous
remodeling, or pressure erosion related to adjacent neurofibromatous
tissue.
Loss or hypoplasia of the sphenoid wing results in widening of the
superior orbital fissure and disruption of the normal barrier between
the orbit and middle cranial fossa. This permits herniation of CSF and
brain parenchyma into the orbit, forming an orbital encephalocele.
Clinically, this manifests as progressive or pulsatile proptosis and may
lead to optic nerve compression, visual impairment, and cosmetic
deformity.
Both cases in this series illustrate a common and clinically
significant diagnostic pitfall: misinterpretation of orbital
encephalocele as an arachnoid cyst. While both entities demonstrate
CSF-like signal intensity on MRI, several imaging features favor
encephalocele, including continuity of herniated brain tissue with
intracranial structures, associated sphenoid wing dysplasia on
CT, displacement of adjacent vascular structures, enlargement or
narrowing of the superior orbital fissure, and the presence of other
NF-1–related findings such as FASI and neurofibromas.
This case series adds to existing literature by emphasizing
that reliance on MRI alone may be insufficient and that CT–MRI
correlation is essential for accurate diagnosis. Prior reports have
similarly highlighted that failure to assess the skull base can delay
diagnosis and appropriate management. Early recognition is clinically
relevant, as progressive orbital encephaloceles may require surgical
reconstruction to prevent irreversible visual loss and significant
cosmetic deformity.
From a management perspective, asymptomatic or slowly
progressive cases may be managed conservatively with close followup,
while patients with visual compromise or rapidly progressive
deformity may benefit from surgical intervention. Accurate diagnosis
therefore directly influences clinical decision-making and patient
outcomes.
Conclusion
Orbital encephalocele secondary to sphenoid wing dysplasia is an
important but under-recognized manifestation of neurofibromatosis
type 1 and a frequent diagnostic mimic of arachnoid cyst. In NF-1
patients presenting with unilateral proptosis, exclusive focus on optic
nerve tumors may lead to misdiagnosis. Careful evaluation of skull
base anatomy with CT–MRI correlation is essential for accurate
diagnosis, appropriate management, and prevention of visual
morbidity.
Acknowledgment
The author gratefully acknowledges the patients and their families
for consenting to publication of this report. The author also sincerely
acknowledges the MRI technician team of the Department of
Radiodiagnosis, Government Medical College, Ernakulam (GMCE),
for their technical expertise and support in acquiring high-quality
imaging studies essential for accurate diagnosis.
References
Citation
Baby NM. Orbital Encephalocele Due to Sphenoid Wing Dysplasia in Neurofibromatosis Type 1: A Case Report Highlighting a Diagnostic Pitfall. Indian J Appl Radiol. 2026;12(1): 225.