Case Report
Trapped in the Fossa: A Case of Left Paraduodenal Hernia
Inchara M, Sandeep Kumar S*, Naveen D, Vishwapremraj DR and Srinivasa Babu CR
Department of Radiodiagnosis, Sapthagiri Institute of Medical Sciences and Research Centre India
*Corresponding author: Dr Sandeep Kumar S, Department of Radiodiagnosis, Sapthagiri Institute of Medical Sciences and Research Centre India. E-mail Id: Sandeepkumars3006@gmail.com
Copyright: ©2026 Inchara M, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information:Submission: 20/11/2025; Accepted: 07/01/2026; Published: 10/01/2026
Abstract
Left paraduodenal hernia (LPDH) is the most common internal hernia and a rare cause of small bowel obstruction, with potential for serious complications if not identified early. We report the case of a 30-year-old male who presented with acute abdominal pain and recurrent vomiting. Contrast-enhanced CT
revealed clustered and dilated jejunal loops in the left paraduodenal region with preserved mural enhancement, and convergence of mesenteric vessels through the hernia neck, findings consistent with LPDH. This case highlights the importance of considering LPDH in young patients with unexplained small
bowel obstruction and underscores the pivotal role of CT in early detection to prevent ischemia and perforation.
Keywords:Left Paraduodenal Hernia; Internal Hernia; Small Bowel Obstruction; Computed Tomography; Exploratory Laparotomy
Introduction
Internal hernias are rare causes of small bowel obstruction,
constituting up to 5.8 % of cases but often leading to strangulation
if undiagnosed [1]. Internal hernias are defined by the herniation
of a viscus through a normal or abnormal peritoneal or mesenteric
aperture within the confines of the peritoneal cavity [2]. Although
historically uncommon, their incidence has been increasing due to
the rise in complex abdominal surgeries such as liver transplantation
and bariatric procedures [1].
Paraduodenal hernia (PDH) represents the most frequent variant of internal hernias, responsible for over 50% of cases [1,2]. PDHs are classified into left and right types, with left paraduodenal hernia (LPDH) being more common [2]. LPDH is characterized by herniation of small intestine into the fossa of Landzert, a space posterior to the inferior mesenteric vein and ascending branch of left colic artery. Ovali et al. described a case of transient LPDH in which small-bowel loops were intermittently seen within this characteristic
Paraduodenal hernia (PDH) represents the most frequent variant of internal hernias, responsible for over 50% of cases [1,2]. PDHs are classified into left and right types, with left paraduodenal hernia (LPDH) being more common [2]. LPDH is characterized by herniation of small intestine into the fossa of Landzert, a space posterior to the inferior mesenteric vein and ascending branch of left colic artery. Ovali et al. described a case of transient LPDH in which small-bowel loops were intermittently seen within this characteristic
location, emphasizing the variable and sometimes reversible
radiologic appearance of this entity [2,3,4,5].
Clinical presentation is often nonspecific, ranging from vague
abdominal pain to acute intestinal obstruction [1,3]. Contrast enhanced
multidetector CT is the diagnostic modality of choice,
as it provides characteristic imaging features and guides surgical
management [4,5].
We present a case of LPDH diagnosed on CT and confirmed
surgically, underscoring the importance of early recognition to
prevent ischemic complications.
Case Report
A 30-year-old male presented to the surgical department with
a one-day history of abdominal pain that was insidious in onset,
gradually progressive, and continuous. The pain was accompanied
by 5–6 episodes of non-projectile vomiting containing food particles.
There was no history of fever, weight loss, diarrhea, or dysuria. On
examination, the patient was hemodynamically stable; abdominal
evaluation revealed diffuse tenderness with guarding, and bowel
sounds were notably muffled on auscultation. The patient reported
a previous episode of jaundice six months earlier, managed
symptomatically, along with similar intermittent abdominal
complaints in the past. Patient was advised erect abdominal
radiogram [Figure 1] which revealed a few localized dilated bowel
loops with air–fluid levels in the left upper paramedian region,
suggestive of localized small bowel obstruction without evidence of
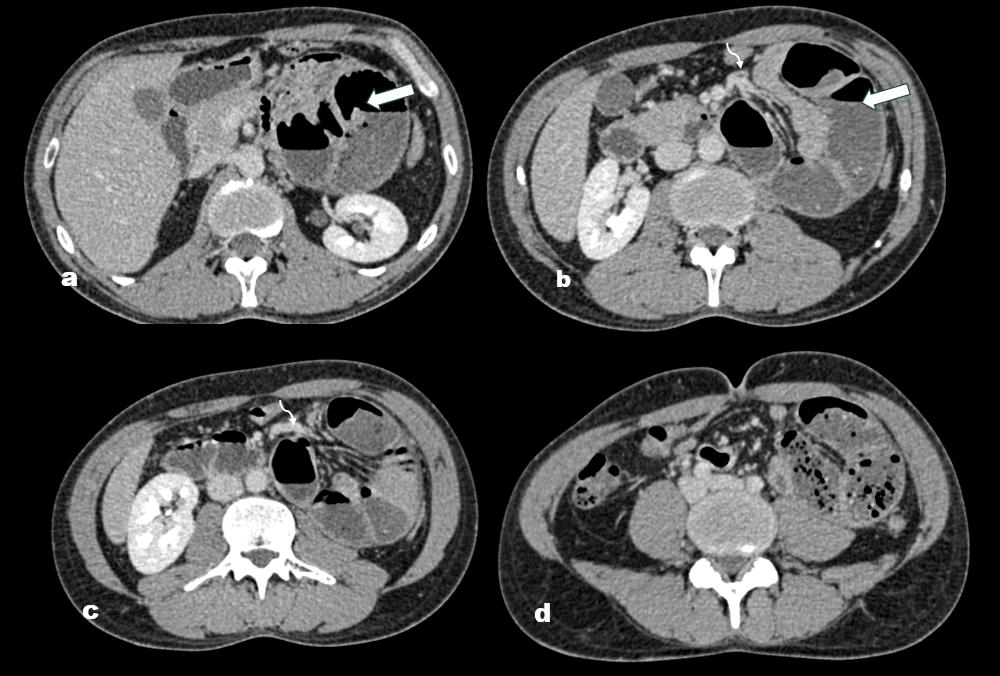
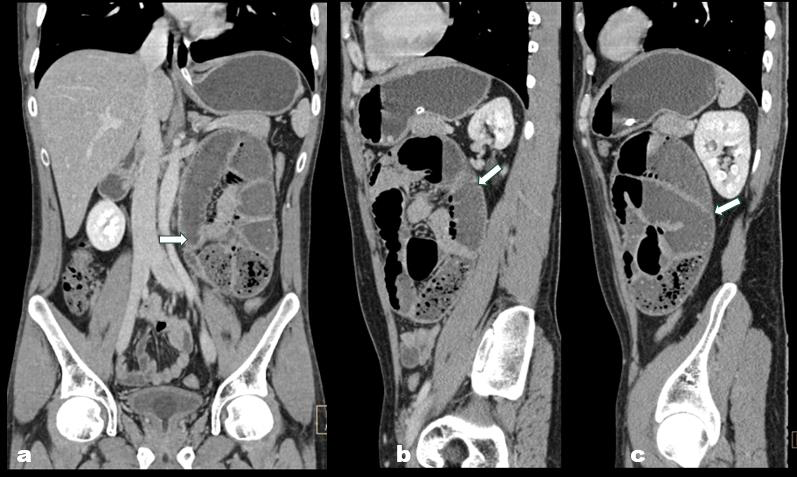
Pneumoperitoneum. For further evaluation, a contrast-enhanced
CT (CECT) scan of the abdomen and pelvis was performed
[Figure 2,3].The study demonstrated clustered and dilated jejunal
loops within the left paraduodenal region, contained in a welldefined
hernia sac, with preserved normal bowel wall enhancement
and normal wall thickness. The mesenteric vessels were observed
to converge and traverse through the hernial neck, without signs
of vascular engorgement, thrombosis, or compression. Considering
the clinical presentation and characteristic radiological findings, a
diagnosis of small bowel obstruction secondary to a left paraduodenal
internal hernia was established. The patient subsequently underwent
exploratory laparotomy and was managed surgically.
Discussion
Paraduodenal hernias were the most common type of internal
hernia, accounting for approximately 53% of all cases [1]. PDH is
further classified into left-sided (approximately 75%) and right sided
(25%) variants. Left paraduodenal hernia (LPDH) results from
incomplete fusion of the descending mesocolon with the posterior
parietal peritoneum, leading to formation of the fossa of Landzert,
a potential space near the duodenojejunal junction through which
bowel loops can herniate [2,3,4,5].
Clinically, paraduodenal hernia typically manifests with nonspecific symptoms, including vague epigastric discomfort, chronic postprandial pain, or recurrent and acute episodes of small bowel obstruction. Some cases may even be discovered incidentally on imaging [1,3,4]. While barium studies historically demonstrated
Clinically, paraduodenal hernia typically manifests with nonspecific symptoms, including vague epigastric discomfort, chronic postprandial pain, or recurrent and acute episodes of small bowel obstruction. Some cases may even be discovered incidentally on imaging [1,3,4]. While barium studies historically demonstrated

characteristic findings such as clustering of small bowel loops and
delayed transit in the left upper abdomen, contrast-enhanced CT has
become the diagnostic modality of choice in modern practice [2,4,5].
On CT, small bowel loops are often clustered in variable locations,
such as adjacent to the duodenojejunal junction, between the stomach
and pancreas, or between the transverse colon and left adrenal gland,
posterior to the pancreatic tail, or within the left anterior pararenal
space. Associated findings include dilated loops with air–fluid
levels, displacement of adjacent viscera, and occasionally stretching,
engorgement, or torsion of mesenteric vessels, which predispose to
ischemia or perforation [1,4,5].
Diagnosis can be challenging due to the intermittent nature of herniation [3]. Spontaneous reduction has been documented in rare instances, initially described on barium studies and later reported in a single CT-documented case [2,3]. This highlights the dynamic character of PDH and emphasizes the need for a high index of suspicion. Prompt surgical intervention is essential, as unresolved obstruction carries a significant risk of morbidity and mortality from ischemia and perforation [1,4,5].
Diagnosis can be challenging due to the intermittent nature of herniation [3]. Spontaneous reduction has been documented in rare instances, initially described on barium studies and later reported in a single CT-documented case [2,3]. This highlights the dynamic character of PDH and emphasizes the need for a high index of suspicion. Prompt surgical intervention is essential, as unresolved obstruction carries a significant risk of morbidity and mortality from ischemia and perforation [1,4,5].
Conclusion
Left paraduodenal hernia, though uncommon, is the most
frequent type of internal hernia and an important cause of small
bowel obstruction in young adults. Its clinical presentation is often
nonspecific, making imaging—particularly CT—vital for diagnosis.
Early recognition is essential, as delayed diagnosis may lead to
ischemia or perforation. Surgical exploration remains the definitive
treatment, with excellent outcomes when performed promptly.
References
Citation
Inchara M, Kumar S, Naveen D, Vishwapremraj DR, Srinivasa Babu CR. Trapped in the Fossa: A Case of Left Paraduodenal Hernia. Indian J Appl Radiol. 2026;12(1): 224.