Case Report
Double Trouble-A Rare Case Report of Unilateral Dichorionic Twin Ectopic Pregnancy
Mudiliyar T and Pereira S*
Department of Radiodiagnosis, Goa Medical College, Goa, India
*Corresponding author:Swizzel Pereira, Department of Radiodiagnosis, Goa Medical College, Goa, India. E-mail Id: swizzelpereira21@gmail.com
Copyright: © 2025 Mudiliyar T, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is
properly cited.
Article Information:Submission: 11/11/2025; Accepted: 12/12/2025; Published: 16/12/2025
Abstract
The incidence of ectopic pregnancies has increased in recent years; however, twin ectopic pregnancies remain extremely rare.
In this case report, we present the clinical and radiological findings of an asymptomatic 38-year-old patient presenting for a routine dating scan in her first trimester. Imaging of this patient revealed the absence of an intrauterine gestational sac with a dichorionic twin ectopic pregnancy in the left adnexa with cardiac activity in both fetal poles. The patient was subsequently taken up for an emergency laparotomy on the same evening, which confirmed a ruptured left ampullary twin gestation; however, hemoperitoneum was absent. The patient underwent left salpingectomy.
Radiologists must recognize the sonographic features of such rare entities to enable timely diagnosis and prevent unwanted complications.
In this case report, we present the clinical and radiological findings of an asymptomatic 38-year-old patient presenting for a routine dating scan in her first trimester. Imaging of this patient revealed the absence of an intrauterine gestational sac with a dichorionic twin ectopic pregnancy in the left adnexa with cardiac activity in both fetal poles. The patient was subsequently taken up for an emergency laparotomy on the same evening, which confirmed a ruptured left ampullary twin gestation; however, hemoperitoneum was absent. The patient underwent left salpingectomy.
Radiologists must recognize the sonographic features of such rare entities to enable timely diagnosis and prevent unwanted complications.
Keywords:Dichorionic Twin Ectopic Pregnancy; Live Ectopic Pregnancy; Transvaginal Ultrasound; Obstetric Emergency
Introduction
Ectopic pregnancy is defined as implantation of a gestational
sac outside the endometrial canal. The most common site for this to
occur is in the fallopian tube (especially in the ampullary segment).
Other sites where the gestational sac can ectopically implant are the
cervix, ovary, rudimentary uterine horn, uterine scars from previous
surgeries, peritoneum, and other abdominal viscera [1]. Ectopic
pregnancies account for 1-2% of all pregnancies, with an increase in
recent years. Contributing factors to their rising incidence include
pelvic inflammatory disease, advancing maternal age, previous tubal
surgeries, and increased use of assisted reproductive technologies.
Here, we describe an additional case of live dichorionic twin ectopic
pregnancy in a primigravida with no predisposing risk factors.
Twin tubal ectopic pregnancies are extremely rare, with only
100 documented case reports, out of which only 8 had the presence
of cardiac activity in the embryos [3]. These pregnancies pose
a significantly higher risk of early tubal rupture with torrential
hemoperitoneum, compared to singleton ectopic pregnancy, due to
the limited distensibility of the fallopian tube.
Patients may present with abdominal pain or bleeding per vaginum, or with symptoms of cardiovascular instability (in case of hemoperitoneum).
Accurate early diagnosis relies heavily on sonological evaluation, particularly transvaginal ultrasound. Identification of multiple extrauterine gestational sacs, their chorionicity, cardiac activity, and their relationship with other adnexal structures is pivotal.
Patients may present with abdominal pain or bleeding per vaginum, or with symptoms of cardiovascular instability (in case of hemoperitoneum).
Accurate early diagnosis relies heavily on sonological evaluation, particularly transvaginal ultrasound. Identification of multiple extrauterine gestational sacs, their chorionicity, cardiac activity, and their relationship with other adnexal structures is pivotal.
Although transvaginal ultrasound is the imaging investigation of
choice, however, trans abdominal ultrasound is useful in screening
the upper abdomen for hemoperitoneum.
Case Presentation
A 38-year-old primigravida presented to the outpatient
department of the obstetrics and gynecology following a positive
urine pregnancy test. The conception was spontaneous. Her LMP was
on 9th September 2025 (corresponding to 7.3 weeks of gestation on
the day of ultrasound). She reported no abdominal pain or vaginal
bleeding/spotting. She had no significant past medical or surgical
history and denied history of pelvic inflammatory disease, use of
intrauterine contraceptive devices, or any infertility treatment. Her
menstrual history revealed no abnormality. She reported a family
history of twin pregnancies in her maternal family.
On examination, the patient was of healthy build, with a normal
BMI. General examination was unremarkable, and the patient was
hemodynamically stable. Per-vaginal examination revealed a slightly
enlarged uterus of approximately 8 weeks size. No forniceal fullness or
adnexal tenderness was documented. The patient was then referred to
the Department of Radiodiagnosis for an ultrasound for the purpose
of dating the pregnancy.
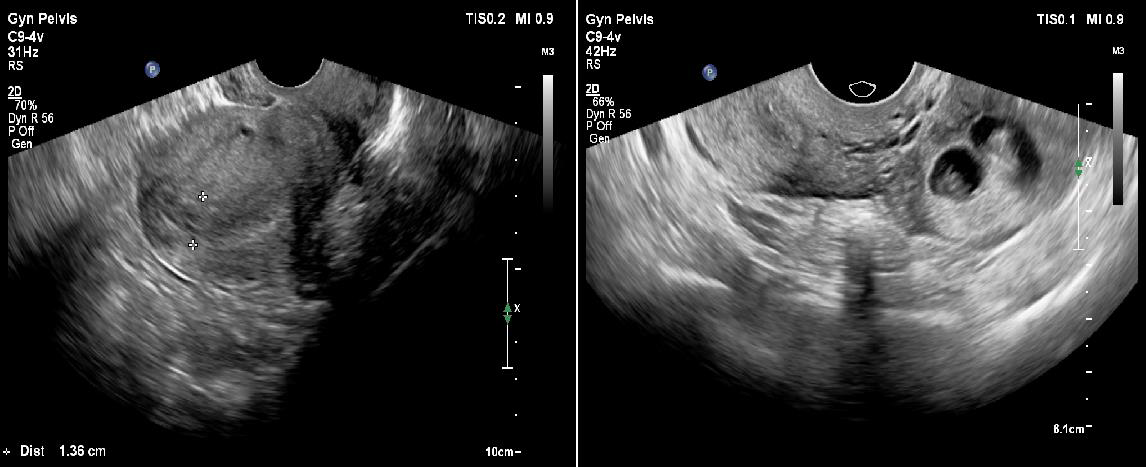
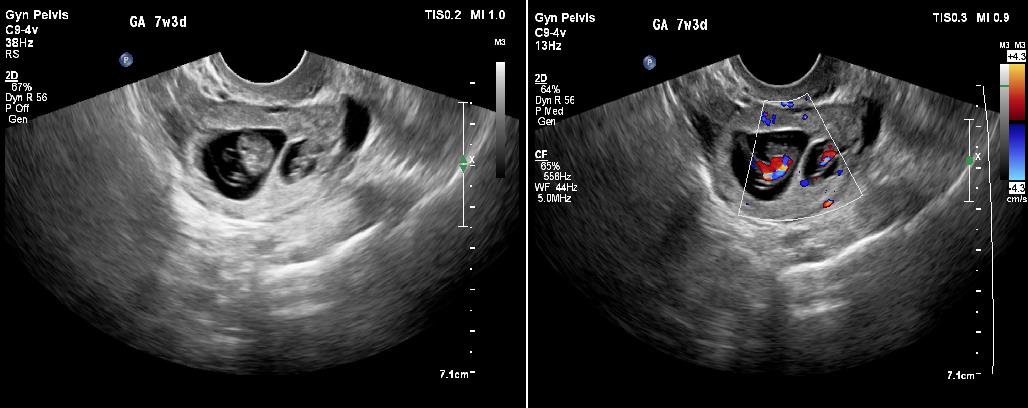
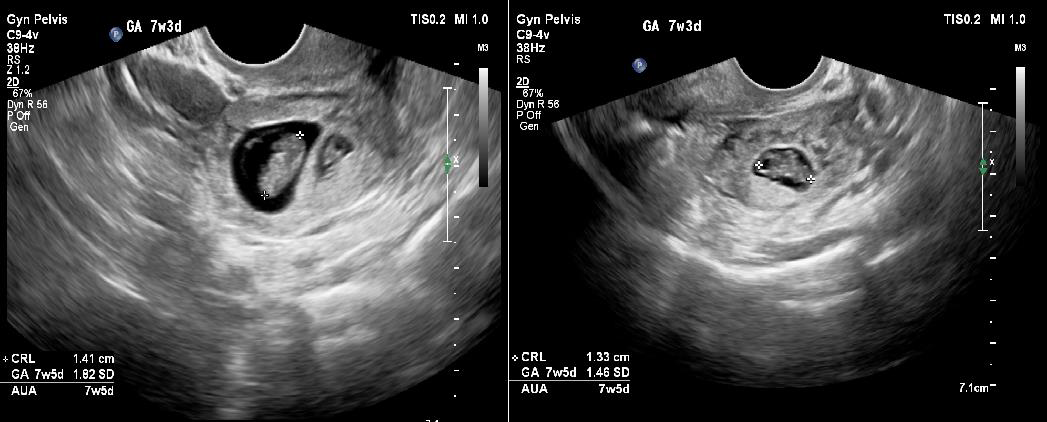
Transabdominal ultrasound revealed a bulky uterus with a thickened endometrium; however, no intrauterine gestational sac was appreciable. A thick-walled cystic structure was noted in the left adnexa with only one fetal pole initially visualized. [Figure 1a and 1b]. Subsequently performed transvaginal ultrasound revealed two gestational sacs in the left adnexa. Twin peak sign was identified, which confirmed dichorionicity. Each gestational sac contained a fetal pole-yolk sac complex [Figure 2a]. Cardiac activity was present in both embryos, confirmed on color Doppler study [Figure 2b]. Crown rump lengths of twin 1 and twin 2 were 13.3 mm and 14.1 mm, respectively, both corresponding to a gestational age of 7.5 weeks each. [Figure 3a and 3b].
Transabdominal ultrasound revealed a bulky uterus with a thickened endometrium; however, no intrauterine gestational sac was appreciable. A thick-walled cystic structure was noted in the left adnexa with only one fetal pole initially visualized. [Figure 1a and 1b]. Subsequently performed transvaginal ultrasound revealed two gestational sacs in the left adnexa. Twin peak sign was identified, which confirmed dichorionicity. Each gestational sac contained a fetal pole-yolk sac complex [Figure 2a]. Cardiac activity was present in both embryos, confirmed on color Doppler study [Figure 2b]. Crown rump lengths of twin 1 and twin 2 were 13.3 mm and 14.1 mm, respectively, both corresponding to a gestational age of 7.5 weeks each. [Figure 3a and 3b].
These gestational sacs were seen separate from but adjacent to the
left ovary, confirming a tubal origin.
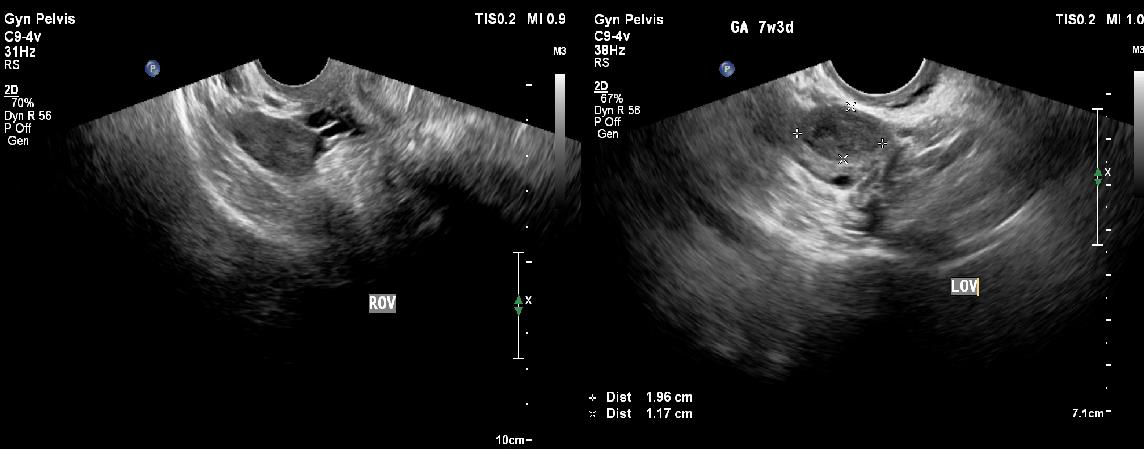
The left ovary showed the presence of a corpus luteum measuring 1.9 x 1.1 cm in size [Figure 4b].
The right ovary and fallopian tube were normal [Figure 4a]. Transvaginal ultrasound also confirmed the absence of an intrauterine gestational sac, thus ruling out a heterotopic pregnancy. Incidentally, a subserosal seedling fibroid was noted in the anterior uterine wall. No free fluid/hemoperitoneum was noted in the abdomen or pelvis at the time of ultrasound.
The obstetricians were immediately notified about this case. The patient underwent an emergency laparotomy under spinal anesthesia. Intra-operatively, a ruptured left ampullary twin ectopic pregnancy was identified. Remarkably, there was no hemoperitoneum despite rupture [Figure 5]. Left salpingectomy was performed. Immediate postoperative period was uneventful. The patient was discharged on postoperative day 3 with appropriately declining serum beta-hCG levels.
The left ovary showed the presence of a corpus luteum measuring 1.9 x 1.1 cm in size [Figure 4b].
The right ovary and fallopian tube were normal [Figure 4a]. Transvaginal ultrasound also confirmed the absence of an intrauterine gestational sac, thus ruling out a heterotopic pregnancy. Incidentally, a subserosal seedling fibroid was noted in the anterior uterine wall. No free fluid/hemoperitoneum was noted in the abdomen or pelvis at the time of ultrasound.
The obstetricians were immediately notified about this case. The patient underwent an emergency laparotomy under spinal anesthesia. Intra-operatively, a ruptured left ampullary twin ectopic pregnancy was identified. Remarkably, there was no hemoperitoneum despite rupture [Figure 5]. Left salpingectomy was performed. Immediate postoperative period was uneventful. The patient was discharged on postoperative day 3 with appropriately declining serum beta-hCG levels.
b)-Transvaginal ultrasound image depicting the extrauterine location of the two gestational sacs in the left adnexa.

Discussion
Ectopic pregnancy is defined as implantation of a gestational sac
outside the endometrial cavity, having an incidence of 1-2% of all
pregnancies. The most common sites for it to occur are the fallopian
tube (90%), ovary, cervix, uterine rudimentary horns, uterine scars
from previous surgeries, peritoneum, and other abdominal organs. In
the fallopian tube, the most common site is the ampullary segment,
accounting for 70% of tubal ectopic pregnancies, followed by the
isthmic segment, the infundibulum, and the intramural segments [1].
The fallopian tube was once thought of as a passive conduit for the released ovum and conceptus, however, this is no longer considered true. The fallopian tube plays an active role in the transportation of the ovum and conceptus to the uterine cavity. This is due to the presence of pseudostratified ciliated columnar epithelium, which lines the tubal mucosa. The cilia beat in the direction of the uterus, thus facilitating transportation. Another factor that helps in transportation is peristalsis of the muscular layer of the tube. Another important factor is the presence of goblet cells, which produce mucous and allow uninterrupted transportation. Diseases that affect any of these factors can potentially lead to a tubal ectopic pregnancy.
The fallopian tube was once thought of as a passive conduit for the released ovum and conceptus, however, this is no longer considered true. The fallopian tube plays an active role in the transportation of the ovum and conceptus to the uterine cavity. This is due to the presence of pseudostratified ciliated columnar epithelium, which lines the tubal mucosa. The cilia beat in the direction of the uterus, thus facilitating transportation. Another factor that helps in transportation is peristalsis of the muscular layer of the tube. Another important factor is the presence of goblet cells, which produce mucous and allow uninterrupted transportation. Diseases that affect any of these factors can potentially lead to a tubal ectopic pregnancy.
The most important risk factors predisposing to ectopic
pregnancies are a history of ectopic pregnancy and previous tubal
surgeries (likely salpingostomy or tubal ligations). Other risk factors
include pelvic inflammatory disease, smoking, endometriosis,
previous pelvic surgeries, and the presence of intrauterine
contraceptive devices, increasing maternal age, and multiple previous
pregnancies [1].
There is a steady rise in the incidence of ectopic pregnancies over recent years owing to a rise in assisted reproductive techniques, as well as an increase in pelvic inflammatory disease, usually secondary to sexually transmitted diseases.
In our case, the patient had no predisposing risk factors and had a spontaneous conception.
Twin tubal ectopic pregnancy is an extremely rare and extremely dangerous subset of ectopic pregnancies with a reported incidence of 1 in 125,000 to 250,000 cases [2]. Among these, spontaneous, unilateral, twin live ectopic pregnancies are extremely uncommon, with only 8 previous documented cases of demonstrable cardiac activity [3].
There is a steady rise in the incidence of ectopic pregnancies over recent years owing to a rise in assisted reproductive techniques, as well as an increase in pelvic inflammatory disease, usually secondary to sexually transmitted diseases.
In our case, the patient had no predisposing risk factors and had a spontaneous conception.
Twin tubal ectopic pregnancy is an extremely rare and extremely dangerous subset of ectopic pregnancies with a reported incidence of 1 in 125,000 to 250,000 cases [2]. Among these, spontaneous, unilateral, twin live ectopic pregnancies are extremely uncommon, with only 8 previous documented cases of demonstrable cardiac activity [3].
The exact pathogenesis by which twin ectopic pregnancy has
occurred is not well understood. One theory suggests synchronous
implantation of two separately fertilized ova in the same tube (which
explains dichorionic twin ectopic). Another theory suggests postimplantation
twinning (which explains monochorionic twins) [3,4].
In our case, two separate gestational sacs were identified with the presence of “delta sign/twin peak sign”, indicating a dichorionic gestation. It must be remembered that dichorionic ectopic gestations may be seen in both fallopian tubes; however, monochorionic gestations will always present unilaterally [3].
Diagnosis of ectopic pregnancy, and by extension, twin ectopic pregnancy, is clinico-radiological [5]. Patients present with the classical triad of amenorrhea, abdominal pain, and bleeding per vaginum; however, not all components of this triad may be encountered. Per vaginal examination often reveals forniceal fullness/ bogginess and tenderness on the affected side. Cervical motion test is often positive. Hemodynamic instability may be seen in the case of ruptured ectopic pregnancy (twin or singleton), presenting as tachycardia and hypotension. These findings, however, were absent in our case. Quantitative serial serum beta HCG reveals elevated HCG levels but a lack of doubling in 48 hours.
Interestingly, our patient was asymptomatic, highlighting the importance of routine early pregnancy imaging and careful adnexal assessment.
In our case, two separate gestational sacs were identified with the presence of “delta sign/twin peak sign”, indicating a dichorionic gestation. It must be remembered that dichorionic ectopic gestations may be seen in both fallopian tubes; however, monochorionic gestations will always present unilaterally [3].
Diagnosis of ectopic pregnancy, and by extension, twin ectopic pregnancy, is clinico-radiological [5]. Patients present with the classical triad of amenorrhea, abdominal pain, and bleeding per vaginum; however, not all components of this triad may be encountered. Per vaginal examination often reveals forniceal fullness/ bogginess and tenderness on the affected side. Cervical motion test is often positive. Hemodynamic instability may be seen in the case of ruptured ectopic pregnancy (twin or singleton), presenting as tachycardia and hypotension. These findings, however, were absent in our case. Quantitative serial serum beta HCG reveals elevated HCG levels but a lack of doubling in 48 hours.
Interestingly, our patient was asymptomatic, highlighting the importance of routine early pregnancy imaging and careful adnexal assessment.
Transvaginal ultrasound is the imaging modality of choice. It
accurately reveals the presence of multiple gestational sacs in one
or both fallopian tubes, their chorionicity, the presence of a fetal
pole-yolk sac complexes, cardiac activity, the presence or absence of
concurrent intrauterine gestational sac, and also trace amounts of
pelvic free fluid/hemorrhage. Transvaginal ultrasound also accurately
demonstrates the location of the adnexal ectopic pregnancy, whether
it’s tubal or ovarian. Color Doppler may be applied to confirm the
presence of cardiac activity and to demonstrate the suggestive of
called “ring of fire”, which is essentially peri-trophoblastic hypervascularity.
Trans abdominal ultrasound is useful in assessing the overview of the abdomen and pelvis before performing a transvaginal ultrasound. It is also used to demonstrate hemoperitoneum in the
upper abdomen. [4,5].
While in most cases, no further imaging modalities may be employed, MRI may be performed in equivocal cases. CT scans are usually not performed; however, they may be performed inadvertently in a female of reproductive age group with abdominal pain under investigation.
Differential diagnosis includes ovarian twin ectopic pregnancy and corpus luteum. In both of these cases, a rim of ovarian tissue will be seen all around them (claw sign). Ring of fire sign, though classically described in ectopic pregnancies, may also be seen around the corpus luteum; however, this ring tends to be more “complete” in the corpus luteum than in an ectopic gestation.
Patients with unilateral twin ectopic pregnancies may be managed medically or surgically.
While in most cases, no further imaging modalities may be employed, MRI may be performed in equivocal cases. CT scans are usually not performed; however, they may be performed inadvertently in a female of reproductive age group with abdominal pain under investigation.
Differential diagnosis includes ovarian twin ectopic pregnancy and corpus luteum. In both of these cases, a rim of ovarian tissue will be seen all around them (claw sign). Ring of fire sign, though classically described in ectopic pregnancies, may also be seen around the corpus luteum; however, this ring tends to be more “complete” in the corpus luteum than in an ectopic gestation.
Patients with unilateral twin ectopic pregnancies may be managed medically or surgically.
Contraindications for medical management include heterotopic
ectopic pregnancy, presence of live embryo, ruptured ectopic
pregnancy, hemodynamic instability, and certain preexisting medical
conditions.
While ectopic pregnancies are considered surgical emergencies on their own, the presence of a unilateral twin ectopic pregnancy greatly increases the risk of tubal rupture earlier than a singleton ectopic pregnancy of the same gestation, due to the limited distensibility of the fallopian tubes. This inadvertently predisposes the mother to earlier as well as greater degrees of hemoperitoneum and maternal mortality [4].
Interestingly, our patient had a ruptured ectopic pregnancy without hemoperitoneum, an uncommon occurrence. Since in our case there was the presence of live embryos, she was surgically managed. Laparoscopy (preferred) or laparotomy may be performed, followed by salpingostomy or salpingectomy [5]. Salpingectomy is generally favoured over salpingostomy due to tubal damage.
In our case, laparotomy followed by left salpingectomy was performed since it was found to be ruptured at the ampullary segment on table.
While ectopic pregnancies are considered surgical emergencies on their own, the presence of a unilateral twin ectopic pregnancy greatly increases the risk of tubal rupture earlier than a singleton ectopic pregnancy of the same gestation, due to the limited distensibility of the fallopian tubes. This inadvertently predisposes the mother to earlier as well as greater degrees of hemoperitoneum and maternal mortality [4].
Interestingly, our patient had a ruptured ectopic pregnancy without hemoperitoneum, an uncommon occurrence. Since in our case there was the presence of live embryos, she was surgically managed. Laparoscopy (preferred) or laparotomy may be performed, followed by salpingostomy or salpingectomy [5]. Salpingectomy is generally favoured over salpingostomy due to tubal damage.
In our case, laparotomy followed by left salpingectomy was performed since it was found to be ruptured at the ampullary segment on table.
Conclusion
Twin ectopic pregnancy is an extremely rare but life-threatening
condition. It predisposes the mother to exponentially greater risks
than those of singleton ectopic pregnancies; hence, extreme vigilance
and knowledge of this entity are important. Its rarity may stun an
unsuspecting radiologist/sonologist. Early and meticulous imaging
is essential as presentations may be subtle. This case highlights
the importance of vigilance during early pregnancy imaging.
Transvaginal ultrasound allows accurate diagnosis and guides
further management. Prompt recognition is vital to reduce maternal
morbidity and mortality.
References
Citation
Mudiliyar T, Pereira S. Double Trouble-A Rare Case Report of Unilateral Dichorionic Twin Ectopic Pregnancy. Indian J Appl Radiol. 2025;11(1): 223.