Case Report
Twist of Fate: A Rare Case of Congenital In-situ Hepatic Malrotation with Diaphragmatic Eventration
Sandeep Kumar S*, Inchara M, Naveen D, Vishwapremraj DR and Srinivasa Babu CR
Department of Radiodiagnosis, Sapthagiri Institute of Medical Sciences and Research Centre, Bengaluru, Karnataka, India
*Corresponding author: Dr Sandeep Kumar S, Department of Radiodiagnosis, Sapthagiri Institute of Medical Sciences and Research Centre, Bangalore, Karnataka, India. E-mail Id Sandeepkumars3006@gmail.com
Copyright: © 2025 Sandeep Kumar S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information:Submission: 14/10/2025; Accepted: 17/11/2025; Published: 21/11/2025
Abstract
Hepatic malrotation is an uncommon developmental anomaly in which the liver and its associated structures occupy an atypical orientation. We present a 46-year-old man with a rare combination of hepatic malrotation and diaphragmatic eventration, identified incidentally during evaluation for chronic abdominal pain. This case adds to the limited published literature, highlighting the challenges in detection and the implications for radiological interpretation and surgical planning. Recognition of this anomaly in adults is particularly important, as it is often overlooked or misinterpreted.
Keywords:Hepatic Malrotation; Diaphragmatic Eventration; Congenital Anomaly
Introduction
Congenital variations of normal liver anatomy are rare. Liver
anomalies can be broadly classified as congenital anomalies or
acquired morphological changes. They may also be categorized
based on the system involved into anatomic hepatic anomalies,
hereditary anomalies, and vascular or biliary system anomalies
[1]. Anatomical anomalies—such as situs abnormalities or atypical
lobation, including accessory lobes—are most often incidental
findings and may be identified in pediatric or adult patients during
imaging studies, surgical procedures, or autopsies. One was in a
patient with antiphospholipid antibody syndrome as an incidental
post-mortem finding by Zhong, [2] and the other in an adult with
congenital diaphragmatic hernia [3,4]. We report a rare case of
hepatic Malrotation with diaphragmatic eventration in an adult,
emphasizing its radiological findings and clinical relevance.
Case Report
A 46-year-old male with a history of HBsAg positivity and pangastritis
presented to the medicine department with complaints of
chronic abdominal pain, not associated with vomiting or loose stools.
The patient reported self-medicating with tramadol daily for the past
6 months and had recently increased the dose due to aggravated pain
over the last week. On examination, the patient was hemodynamically
stable with mild diffuse abdominal tenderness. Laboratory
investigations were normal. An ultrasound scan performed elsewhere
had reported bilateral renal calculi. A contrast-enhanced CT (CECT)
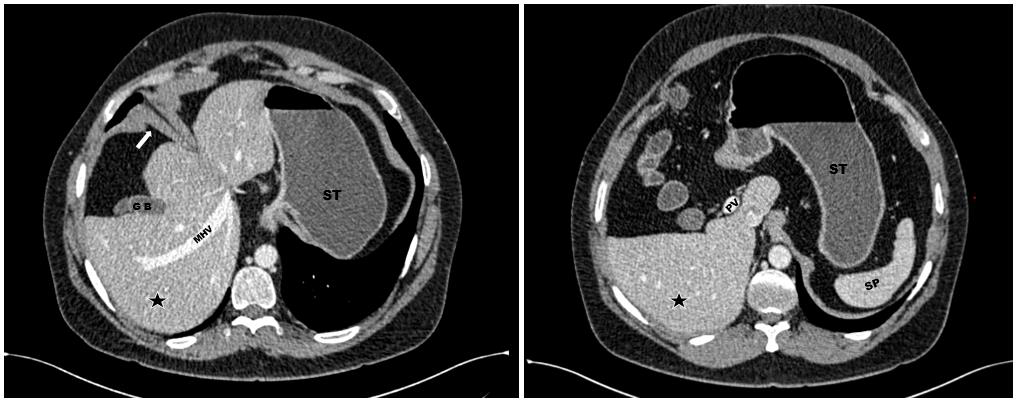
of the abdomen was advised for further evaluation. The CT study
demonstrated a malrotated liver with the hepatic hilum oriented
anterolaterally and the gallbladder located in an atypical anterior
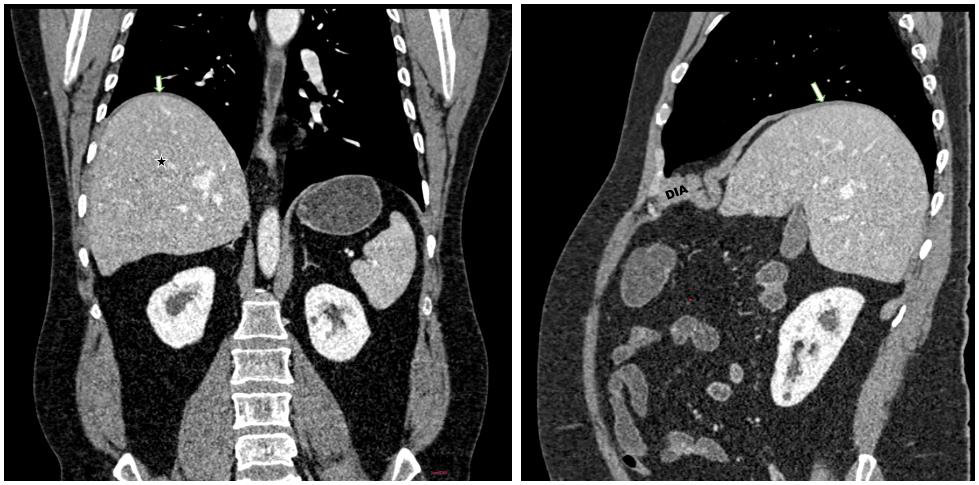
position [Figure 1] There was moderate to marked elevation of the
posterior aspect of the right hemidiaphragm along with upward
displacement of the right hepatic lobe, suggesting diaphragmatic
eventration [Figure 2]. Additionally, a right-sided partial duplex
collecting system with microliths in the mid-pole of the right kidney
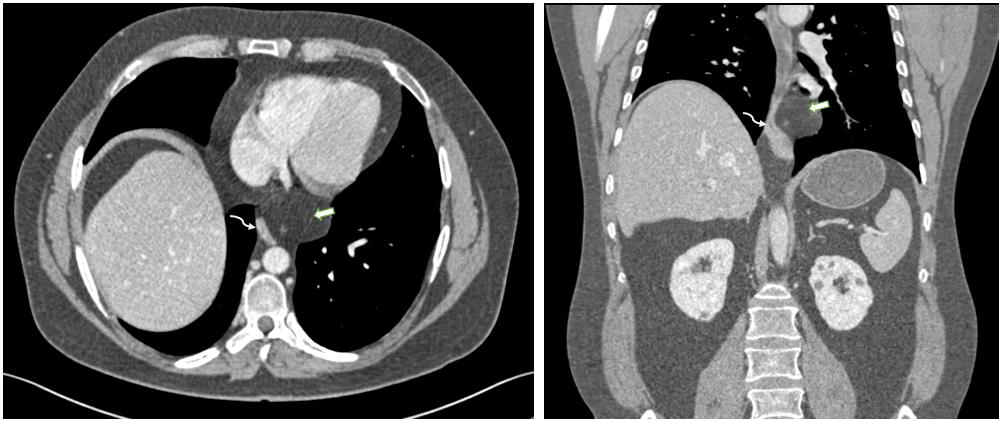
was demonstrated. Diffuse fat deposition was noted around the lower
esophagus, pericardium, and visualized mediastinum, indicative
of mediastinal lipomatosis an incidental finding. No evidence of
other associated findings like dextrocardia, polysplenia or asplenia,
intestinal malrotation and heterotaxy syndrome was identified. The
patient was managed conservatively with antispasmodics and proton
pump inhibitors for symptomatic relief, and a psychiatric opinion
was sorted for tramadol addiction but subsequently patient was lost
to follow-up.
Discussion
Hepatic malrotation is a very uncommon congenital anomaly
in which the liver fails to assume its expected orientation during
embryonic development. Anatomical anomaly in the adult liver is a
very rare occurrence. Most of them usually involve a part of the liver,
a lobe, or segments that present with agenesis or fusion [2].
During the mid-third to early fourth week of embryonic development, the hepatic diverticulum emerges from the distal foregut as an endodermal outgrowth. After penetrating the septum transversum, the liver bud divides into right and left components, which subsequently give rise to the individual lobes. The pars cystica—destined to form the gallbladder and cystic duct—arises as a ventral outpouching from the developing bile ducts. Initially, the bile duct opens ventrally into the developing duodenum; following gut rotation, it assumes a dorsal opening. Anatomical variations of the liver are rare and are usually detected incidentally, with most exerting no significant physiological or functional impact. Among these, lobar or segmental agenesis and fusion represent the predominant forms [3].
Recognizing various anatomical abnormalities of the liver will benefit clinical practice, especially valuable for radiologists and surgeons [2]. Advanced diagnostic imaging modalities play a major role in medical practice. Especially, understanding the normal liver anatomy [1,5] or variants for treating interventionists, surgeons, and interpreting radiologists [1]. This report documents one of the very few adult cases of hepatic malrotation described in the literature, highlighting the importance of recognizing such anomalies to ensure accurate diagnosis and safe clinical management.
During the mid-third to early fourth week of embryonic development, the hepatic diverticulum emerges from the distal foregut as an endodermal outgrowth. After penetrating the septum transversum, the liver bud divides into right and left components, which subsequently give rise to the individual lobes. The pars cystica—destined to form the gallbladder and cystic duct—arises as a ventral outpouching from the developing bile ducts. Initially, the bile duct opens ventrally into the developing duodenum; following gut rotation, it assumes a dorsal opening. Anatomical variations of the liver are rare and are usually detected incidentally, with most exerting no significant physiological or functional impact. Among these, lobar or segmental agenesis and fusion represent the predominant forms [3].
Recognizing various anatomical abnormalities of the liver will benefit clinical practice, especially valuable for radiologists and surgeons [2]. Advanced diagnostic imaging modalities play a major role in medical practice. Especially, understanding the normal liver anatomy [1,5] or variants for treating interventionists, surgeons, and interpreting radiologists [1]. This report documents one of the very few adult cases of hepatic malrotation described in the literature, highlighting the importance of recognizing such anomalies to ensure accurate diagnosis and safe clinical management.
Conclusion
This case highlights the critical importance of recognizing
rare anatomical variations, such as hepatic malrotation, in clinical
practice. Comprehensive preoperative imaging plays a pivotal
role in ensuring accurate diagnosis, guiding surgical planning,
and preventing intraoperative complications. Awareness of such
anomalies is essential for radiologists and surgeons alike to optimize
patient care and outcomes.
References
Citation
Sandeep Kumar S, Inchara M, Naveen D, Vishwapremraj DR, Srinivasa Babu CR. Twist of Fate: A Rare Case of Congenital In-situ Hepatic Malrotation with Diaphragmatic Eventration. Indian J Appl Radiol. 2025;11(1): 222.