Case Report
A Case Report and Imaging Review of An Uncommon Case of Tuberculous Dactylitis In An Adult
Pathapati D*, Chandh JS, Gudelli Rajesh K, Asif Mohd and Jyothsna K
Department of Radiology, KIMS hospital enterprises pvt.ltd, Kondapur, Hyderabad, Telangana, India.
*Corresponding author:Dr. Deepthi Pathapati, Department of Radiology, KIMS hospital enterprises pvt.ltd, Kondapur, Hyderabad, Telangana, India. E-mail id: deepthipathapati82@gmail.com
Copyright: © 2025 Pathapati D, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information:Submission: 24/09/2025; Accepted: 27/10/2025; Published: 31/10/2025
Abstract
Tuberculous dactylitis, a rare form of osteoarticular tuberculosis (TB), affects the short tubular bones of the hands and feet, such as the phalanges, metacarpals, and metatarsals. This condition is more frequently observed in the hands than the feet and is exceptionally rare in individuals older than five
years. The diagnosis of tuberculous dactylitis is often challenging due to its atypical presentation, limited diagnostic methods, and its similarities with other diseases. This case report describes a rare instance of tuberculous dactylitis in an adult patient with no identifiable risk factors, who was successfully treated
with anti-tubercular medication, highlighting the need for increased awareness and accurate diagnostic approaches.
Keywords:Tuberculous Dactylitis; Osteoarticular Tuberculosis; Spina Ventosa; Tuberculous Osteitis.
Introduction
Tuberculous dactylitis is an uncommon manifestation of
tuberculosis that primarily affects the short tubular bones in the hands
and feet, including the phalanges, metacarpals, and metatarsals. This
form of skeletal tuberculosis, while constituting a minor portion
(2–4%) of skeletal TB cases, is particularly rare compared to other
forms. Although osteoarticular TB accounts for a small fraction (1-
3%) of all TB infections, tuberculous dactylitis constitutes only 2–4%
of skeletal TB cases. It generally affects the hands more than the feet
and is seldom seen in individuals over five-year-old.
Diagnosing tuberculous dactylitis presents significant difficulties due to its rare presentation, challenges in diagnostic techniques, and the overlap with other medical conditions. This article explores a rare case of tuberculous dactylitis in an adult patient, emphasizing the importance of thorough diagnostic evaluation and effective treatment with anti-tubercular therapy.
Diagnosing tuberculous dactylitis presents significant difficulties due to its rare presentation, challenges in diagnostic techniques, and the overlap with other medical conditions. This article explores a rare case of tuberculous dactylitis in an adult patient, emphasizing the importance of thorough diagnostic evaluation and effective treatment with anti-tubercular therapy.
Case Report
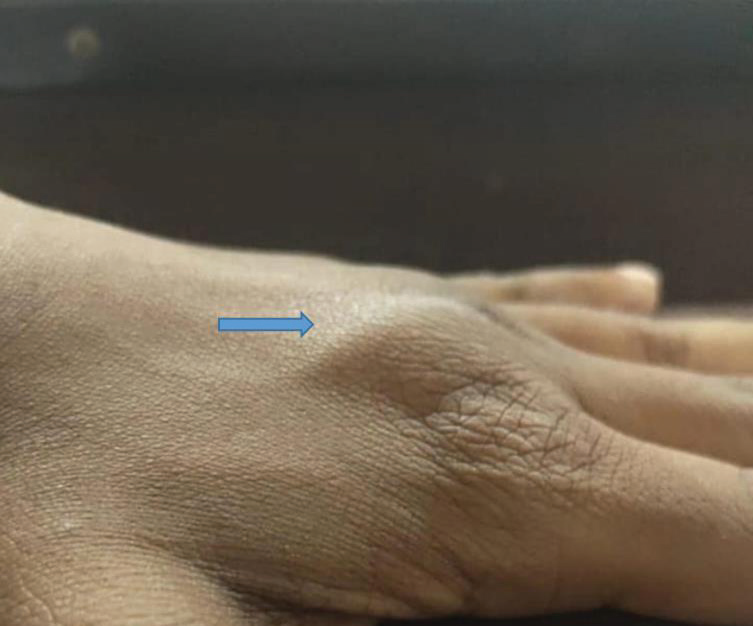
We present a case involving a 19-year-old male who came with a
complaint of swelling on the dorsum of his left hand, present for two
months. The patient had been asymptomatic until two months prior
when he noticed a gradually progressive swelling at the base of the
third digit. The swelling appeared insidiously and was not associated
with any pain. There was no reported history of trauma, cough,
weight loss, decreased appetite, or other risk factors. The patient
had previously received antibiotic treatment at other healthcare
facilities. Upon examination, a firm, rounded swelling was observed
at the base of the third digit [Figure 1]. There were no signs of local
inflammation, although the range of motion in the affected finger was
painful and limited.
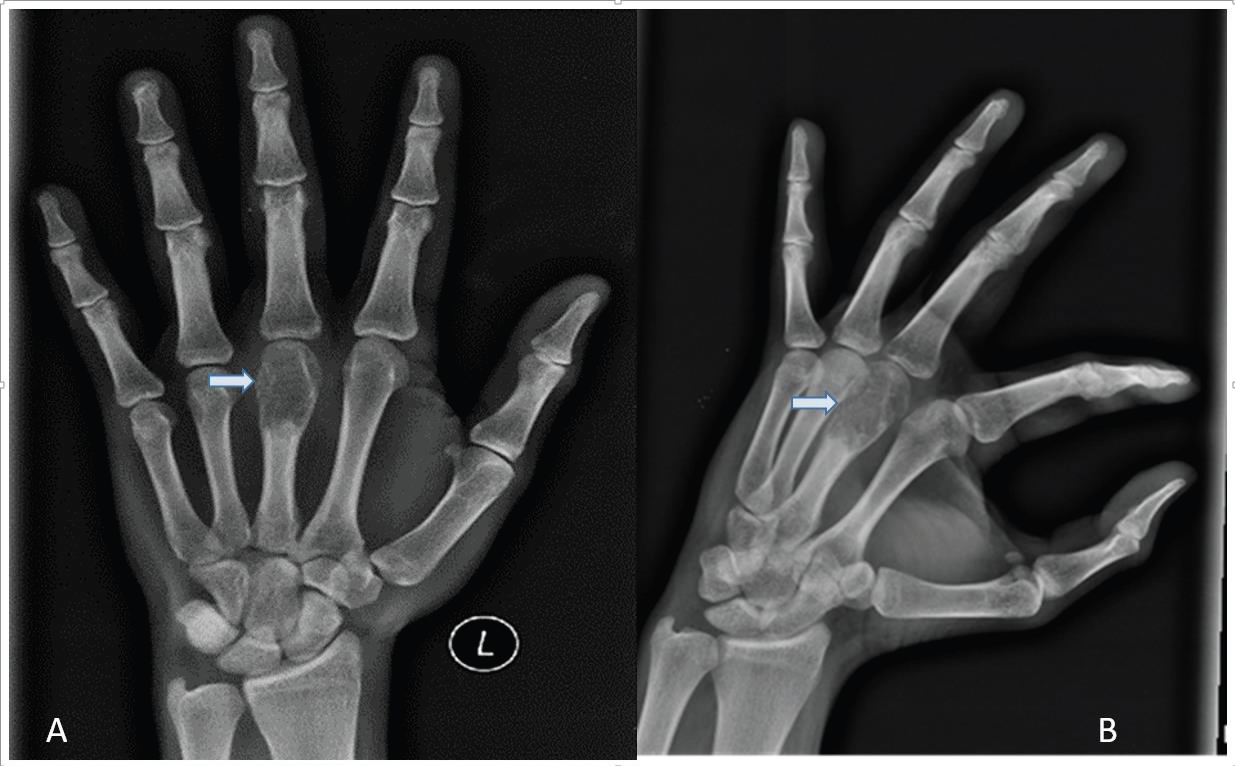
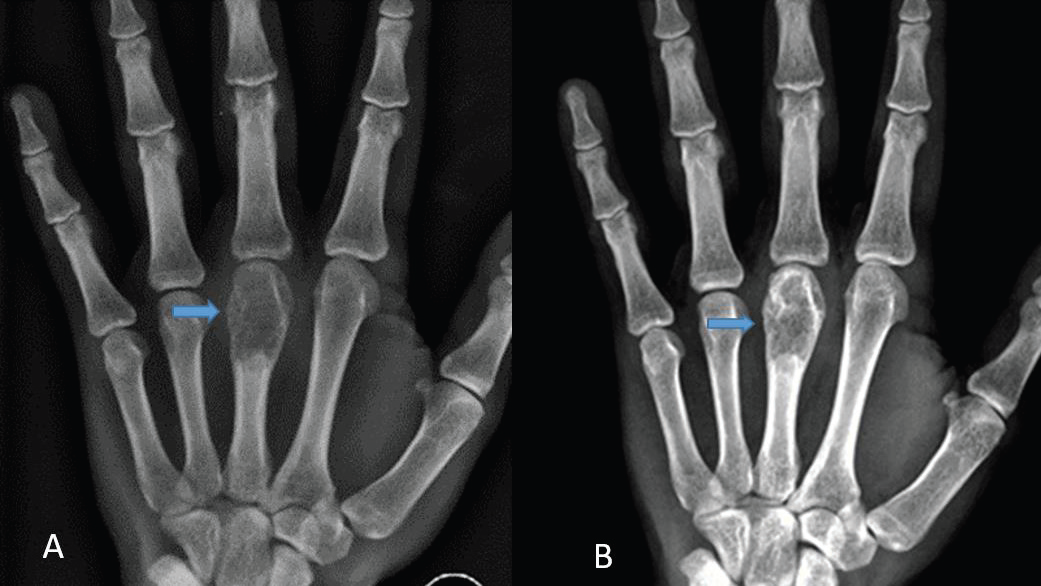
AP Radiograph of left hand revealed a mild expansile lytic lesion with thin septations and a narrow zone of transition, involving the head and proximal shaft of the third metacarpal bone, without periosteal reaction or soft tissue involvement [Figure 2]. The differential diagnosis considered were enchondroma, aneurysmal bone cyst, and tuberculous dactylitis.
AP Radiograph of left hand revealed a mild expansile lytic lesion with thin septations and a narrow zone of transition, involving the head and proximal shaft of the third metacarpal bone, without periosteal reaction or soft tissue involvement [Figure 2]. The differential diagnosis considered were enchondroma, aneurysmal bone cyst, and tuberculous dactylitis.
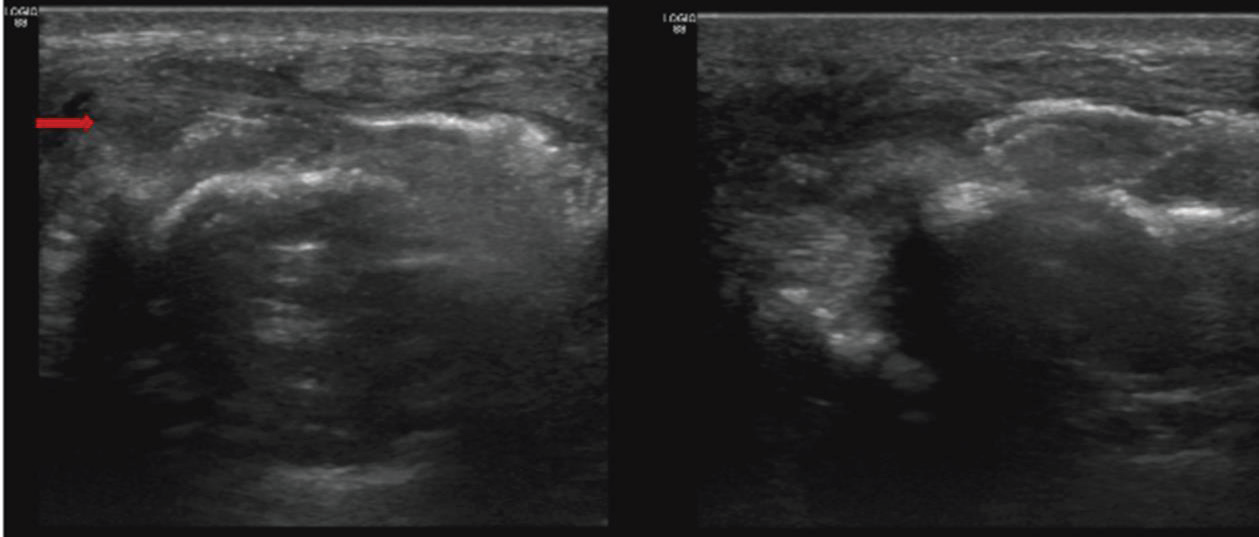
Given the lytic expansile lesion and the presence of adjacent soft
tissue, the clinician recommended a guided biopsy. An ultrasound
(USG) showed the bone lesion with associated soft tissue component
[Figure 3].Under aseptic precaution and local anesthesia ultrasound
guided percutaneous core needle biopsy of the lesion was performed
using a co axial 18-gauge semi-automated biopsy gun. The procedure
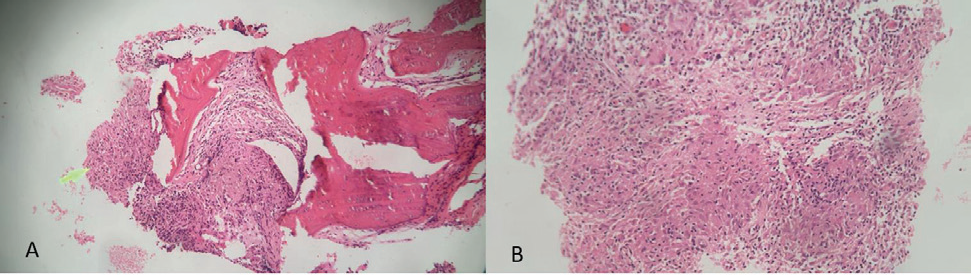
was uneventful. Histopathological examination (HPE) of the
obtained tissue confirmed necrotizing granulomatous osteomyelitis
due to tuberculosis [Figure 4].
Following the diagnosis, anti-tubercular therapy (ATT) was
initiated. At the six-month follow-up, radiographic evaluation
showed a reduction in soft tissue swelling clinically, a slight decrease
in the lytic component, and increased sclerosis of the lesion [Figure 5].
Discussion
Tuberculous dactylitis, a rare form of skeletal tuberculosis,
affects the short tubular bones of the hands and feet, such as the
metatarsals, metacarpals, and phalanges. This condition represents
a minor fraction (2–4%) of skeletal TB cases and most commonly
results from hematogenous dissemination of tuberculosis from the
lungs [1,2]. Over 85% of cases affect children with the hands being
more commonly affected than the feet [1]. It is more frequently
observed in the fingers rather than the toes, with the proximal
phalanx of the index and middle fingers being the most commonly
involved areas. This disease is rare in individuals older than five
years and typically becomes symptomatic 1-3 years post-infection2.
In children, tuberculous dactylitis often involves multiple bones due
to the abundant blood supply in the tubular bones, leading to the
formation of tuberculous granulomas [2]. When the nutrient artery
of the affected bone becomes occluded, a sequestrum forms, resulting
in endosteal destruction and new bone formation. Radiologically, this
condition is termed “spina ventosa” due to its characteristic cystic
expansion appearance.
Clinically, tuberculous dactylitis manifests as a chronic, painful swelling of the digits, primarily affecting the proximal phalanx and metacarpals. It is more severe in children or those with immune deficiencies, where multifocal involvement, sequestration, and complications such as abscesses and secondary bacterial infections
Clinically, tuberculous dactylitis manifests as a chronic, painful swelling of the digits, primarily affecting the proximal phalanx and metacarpals. It is more severe in children or those with immune deficiencies, where multifocal involvement, sequestration, and complications such as abscesses and secondary bacterial infections
are more common. Radiographic imaging typically shows osteolytic
lesions with minimal periosteal reaction, bone sclerosis, and
destruction [1,2]. MRI is particularly useful for detecting early
marrow and soft-tissue involvement and can reveal features like
honeycombing, diffuse infiltration, or cystic lesions. The condition’s
rare presentation without detectable tuberculosis contagion or
immunosuppression is highlighted in this case.
Diagnosis primarily relies on histopathological analysis of biopsy
samples, detection of Mycobacterium tuberculosis through Gene-
Xpert studies, and Ziehl-Neelsen (Z-N) staining for acid-fast bacilli
[2]. Culturing Mycobacterium from bone tissue is the definitive
diagnostic method. Routine laboratory tests, including white blood
cell counts and inflammatory markers, are not diagnostic but can
help rule out other conditions. Treatment involves a prolonged
course of anti-tubercular drugs: isoniazid, rifampicin, pyrazinamide,
and ethambutol for two months, followed by isoniazid and rifampicin
for 6–12 months. Most patients show excellent responses to therapy,
though joint ankylosis can be a significant complication. The
condition is typically well-managed with chemotherapy, resulting in
complete remission in most cases.
Imaging plays a crucial role in diagnosing tuberculous dactylitis,
with radiographic findings helping to differentiate it from other
musculoskeletal infections3. Previous studies have emphasized
the importance of advanced imaging modalities such as MRI and
CT in the detection of early disease and assessing the extent of
bone involvement. According to Vuyst et al., imaging features of
musculoskeletal tuberculosis, including tuberculous dactylitis,
demonstrate characteristic bone destruction and periosteal reaction,
which are instrumental in differentiating it from other pathologies
[4]. The utility of CT imaging for assessing bone changes in advanced
stages of the disease is also well-documented, offering clear insights
into the structural integrity of the affected bones.
Furthermore, Harisinghani et al. highlight the significant role
of radiographic imaging in diagnosing tuberculosis across various
body sites, including the musculoskeletal system. They outline
the radiographic patterns, such as “spina ventosa” in tuberculous
dactylitis,that can help clinicians make an early diagnosis of skeletal
tuberculosis [5]. In adult cases, as discussed by Feldman et al.,
tuberculous dactylitis presents more subtly, and early detection
remains challenging due to less typical clinical symptoms and a
slower progression compared to pediatric cases [6]. Their findings
underscore the importance of a high clinical suspicion and the use
of imaging techniques to identify and confirm the diagnosis of this
rare condition.
Conclusion
Tuberculous dactylitis, while rare, poses significant diagnostic
challenges due to its atypical presentation and the need for
distinguishing it from other conditions. The condition’s diagnostic
process involves a combination of histopathology, advanced imaging,
and microbiological studies. Accurate diagnosis and prompt
treatment with a comprehensive anti-tubercular regimen are crucial
for effective management and recovery. Despite the potential for
complications such as joint ankylosis, most patients respond well to
treatment and achieve complete remission.
The differential diagnosis for this condition includes several possibilities: Chronic pyogenic osteomyelitis, Syphilitic dactylitis, fungal dactylitis, and bone lesions such as enchondroma or fibrous defects. In cases of pyogenic osteomyelitis of the fingers, one should be alert to symptoms such as localized warmth, significant tenderness, high fever, and impaired finger movement accompanied by elevated white blood cell counts. Tuberculous dactylitis typically follows a more indolent course and rarely presents with systemic symptoms [2]. Key differentiators from pyogenic infections include the absence of sequestration and the presence of diffuse osteopenia in tuberculous dactylitis.
The differential diagnosis for this condition includes several possibilities: Chronic pyogenic osteomyelitis, Syphilitic dactylitis, fungal dactylitis, and bone lesions such as enchondroma or fibrous defects. In cases of pyogenic osteomyelitis of the fingers, one should be alert to symptoms such as localized warmth, significant tenderness, high fever, and impaired finger movement accompanied by elevated white blood cell counts. Tuberculous dactylitis typically follows a more indolent course and rarely presents with systemic symptoms [2]. Key differentiators from pyogenic infections include the absence of sequestration and the presence of diffuse osteopenia in tuberculous dactylitis.
Acknowledgment
We sincerely thank the patient for his cooperation and trust
throughout the diagnostic and follow up process. We also extend our
gratitude to the consultants of radiology and orthopedic department
for their dedicated support and expertise, which were vital in
diagnosing and managing this case.
References
Citation
Pathapati D, Chandh JS, Gudelli Rajesh K, Asif Mohd, Jyothsna K. A Case Report and Imaging Review of An Uncommon Case of Tuberculous Dactylitis In An Adult. Indian J Appl Radiol. 2025;11(1): 221.