Case Report
Crossed Testicular Ectopia (CTE) Associated with Persistent Mullerian Duct Syndrome (PMDS): Case Report with Review of Literature
Jyoti Narayan*, Shraddha R. Sinhasan, Shrinivas B Desai, Ritu Kashikar, Chandresh O. Karnawat and Shruti S. Rathod
Department of Radiology, Clinical Associate at Jaslok Hospital and Research Centre, Mumbai, Maharashtra, India
*Corresponding author: Jyoti N, Department of Radiology, Clinical Associate at Jaslok Hospital and Research Centre, Mumbai, Maharashtra, India. E-mail Id: jyoti119@gmail.com
Copyright: ©2025 Jyoti N, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information: Submission: 07/08/2025; Accepted: 29/09/2025; Published: 03/10/2025
Abstract
Crossed testicular ectopia (CTE) is an uncommon congenital anomaly where one testis migrates to the contralateral scrotum. It is often associated with genitourinary anomalies, particularly persistent Müllerian duct syndrome (PMDS). PMDS occurs due to defective anti-Müllerian hormone (AMH) secretion
or receptor response, leading to the persistence of Müllerian derivatives such as the uterus and fallopian tubes in phenotypic males. This association is observed in 20–30% of CTE cases and may be overlooked radiologically. Early diagnosis is crucial because both ectopic testes and Müllerian remnants are
predisposed to malignant transformation.
We present a case of a one-year-old male with unilateral scrotal swelling and an impalpable contralateral testis. MRI revealed bilateral testes on the same (right) side and an additional soft tissue suggestive of a Müllerian structure. Surgical exploration confirmed CTE with PMDS, and management involved orchidopexy with excision of Müllerian remnants.
This case underscores the importance of high-resolution imaging, particularly MRI, for accurate diagnosis of complex gonadal anomalies and highlights the need for early surgical intervention to prevent long-term complications such as malignancy and infertility.
We present a case of a one-year-old male with unilateral scrotal swelling and an impalpable contralateral testis. MRI revealed bilateral testes on the same (right) side and an additional soft tissue suggestive of a Müllerian structure. Surgical exploration confirmed CTE with PMDS, and management involved orchidopexy with excision of Müllerian remnants.
This case underscores the importance of high-resolution imaging, particularly MRI, for accurate diagnosis of complex gonadal anomalies and highlights the need for early surgical intervention to prevent long-term complications such as malignancy and infertility.
Keywords:Crossed testicular ectopia; Persistent Müllerian duct syndrome; Testicular ectopia; Müllerian remnants; Pediatric urology
Introduction
Crossed testicular ectopia (CTE), also known as transverse
testicular ectopia, is a rare congenital anomaly in which both testes
descend through the same inguinal canal. Fewer than 150 cases have
been documented worldwide. It frequently coexists with additional
urogenital anomalies such as inguinal hernia, hypospadias, and
persistent Müllerian duct syndrome (PMDS)[1,2].
PMDS is a disorder of sexual differentiation seen in genotypic males (46, XY) due to a defect in AMH secretion or receptor function.
PMDS is a disorder of sexual differentiation seen in genotypic males (46, XY) due to a defect in AMH secretion or receptor function.
This failure of Müllerian duct regression results in persistence of
structures such as the uterus and fallopian tubes [4]. Though typically
asymptomatic, these remnants have oncological implications. Thus,
early detection and excision are essential.
We report a rare case of CTE associated with PMDS in a one year- old boy, highlighting the critical role of MRI in diagnosis and surgical planning.
We report a rare case of CTE associated with PMDS in a one year- old boy, highlighting the critical role of MRI in diagnosis and surgical planning.
Case Report
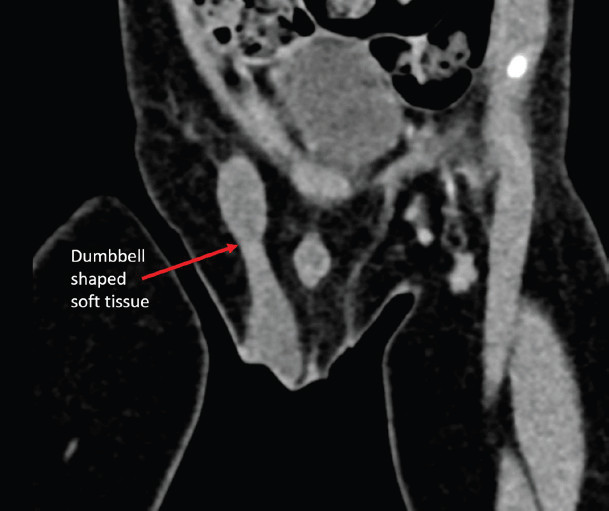
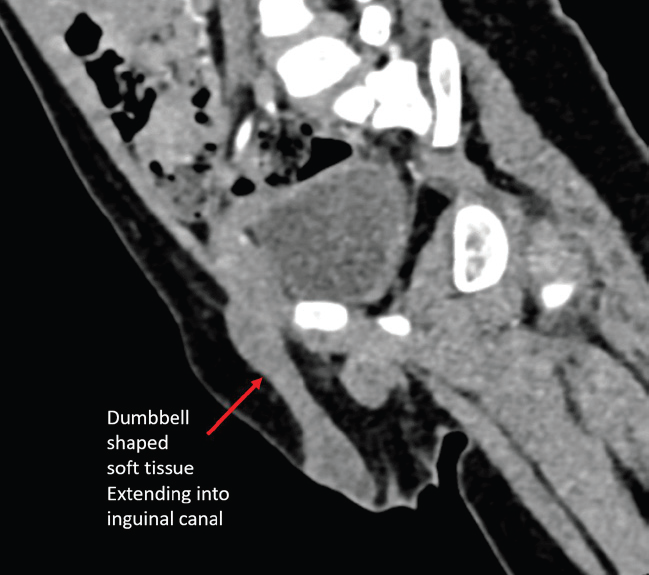
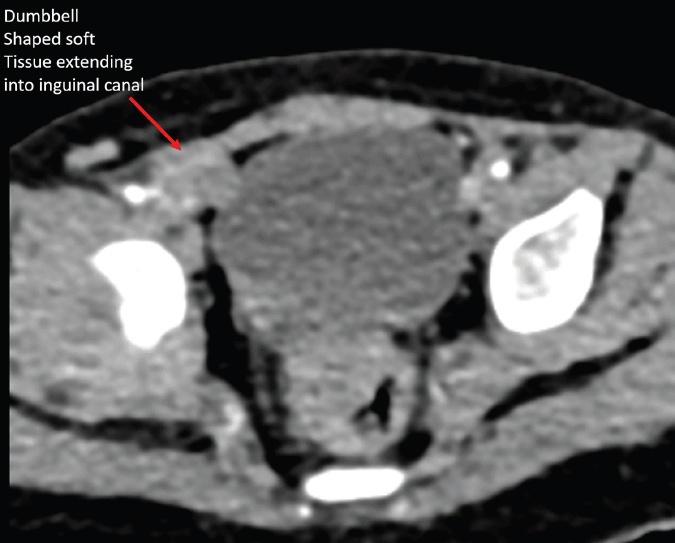
A one-year-old male presented with right scrotal swelling and an
absent left testis on physical examination. Repeated ultrasonography
failed to identify the left testis. Contrast-enhanced CT (CECT) pelvis
revealed a dumbbell-shaped enhancing soft tissue density extending
from the right inguinal canal into the scrotum [Figure 1,2,3].
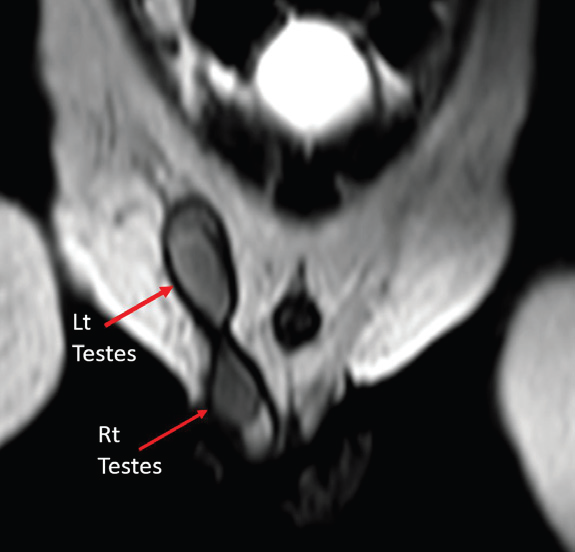
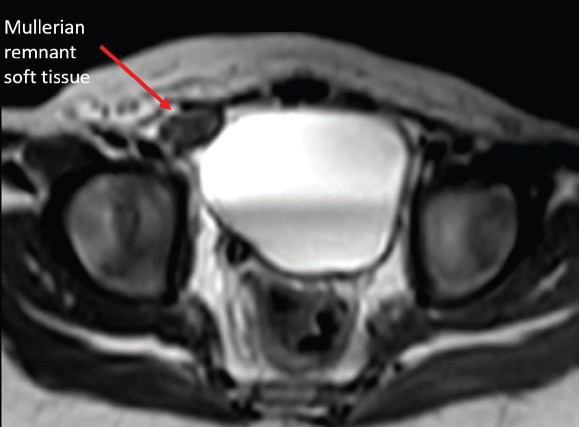
MRI pelvis was performed for soft tissue characterization. T2- weighted sequences demonstrated two testes on the right side—one within the scrotum and the other at the superficial inguinal ring. The ectopic left testis was smaller than the right testis. Additionally, an intermediate-signal-intensity structure was noted in the right inguinal canal, distinct from both testes, suggestive of a Müllerian derivative [Figure 4-6].
MRI pelvis was performed for soft tissue characterization. T2- weighted sequences demonstrated two testes on the right side—one within the scrotum and the other at the superficial inguinal ring. The ectopic left testis was smaller than the right testis. Additionally, an intermediate-signal-intensity structure was noted in the right inguinal canal, distinct from both testes, suggestive of a Müllerian derivative [Figure 4-6].
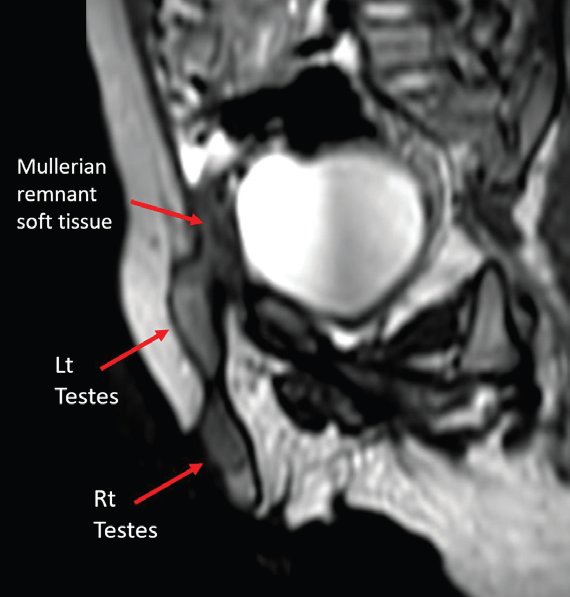
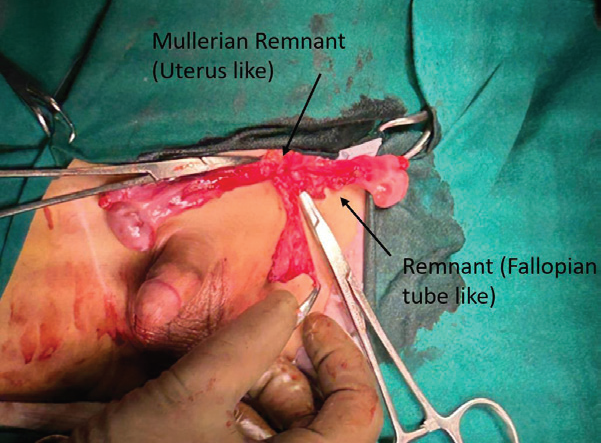
Surgical exploration confirmed bilateral testes on the right side,
with a rudimentary uterus situated between them [Figure 7]. The
Müllerian remnants were excised, and orchidopexy was performed
using an Arabic figure-of-eight technique. The postoperative course
was uneventful.
Discussion
CTE is classified into three types: Type 1 (associated with
inguinal hernia alone), Type 2 (with PMDS), and Type 3 (with
other genitourinary anomalies) [5]. Our case represents Type 2,
characterized by the coexistence of CTE and PMDS.
Embryology and Pathogenesis
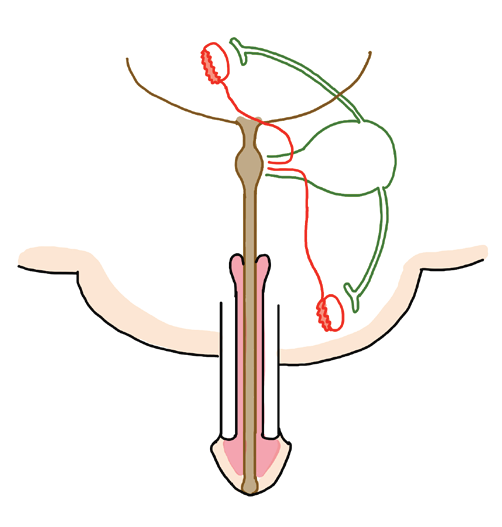
The Müllerian ducts normally regress in males under the influence of AMH secreted by Sertoli cells. In PMDS, either due to AMH gene mutation or receptor defect, regression fails, leading to persistence of Müllerian derivatives [4]. These structures may migrate along with the testes or remain intra-abdominal, sometimes hindering testicular descent [6].
Embryology and Pathogenesis
The Müllerian ducts normally regress in males under the influence of AMH secreted by Sertoli cells. In PMDS, either due to AMH gene mutation or receptor defect, regression fails, leading to persistence of Müllerian derivatives [4]. These structures may migrate along with the testes or remain intra-abdominal, sometimes hindering testicular descent [6].
Imaging and Diagnostic Importance:
Ultrasonography is the first-line investigation for non-palpable
testes but has limitations in detecting intra-abdominal gonads or
associated anomalies. MRI, with its superior soft tissue resolution, is
the modality of choice when CTE or additional soft tissue is suspected.
Typical MRI features of PMDS include [3].
• Uterine-like midline soft tissue between testes
• Band-like fibrous structures
• Tubular structures resembling fallopian tubesClinical Implications and Management:
The risk of malignancy is approximately 18% in ectopic testes and
also significant in Müllerian remnants [7,8]. Reported tumors include
seminomas, embryonal carcinoma, and rare adenocarcinomas [6].
Additional complications include infertility, urinary tract infections,
hematuria, and stone formation [6].Surgical management consists of orchidopexy to position the testes within the scrotum and complete excision of Müllerian remnants to prevent malignant transformation and mechanical complications. Laparoscopy is often the preferred approach for both diagnosis and treatment.
Why Early Detection Matters:
Delayed diagnosis increases the risk of gonadal malignancy and
compromises fertility. Therefore, prompt evaluation with MRI when
CTE is suspected is vital. Our case adds to the limited Indian literature
on CTE with PMDS and emphasizes multidisciplinary management
involving radiologists, pediatric surgeons, and urologists.Conclusion
CTE with PMDS, though rare, is clinically significant due to
its oncological implications. MRI should be considered in all cases
of non-palpable testes when ultrasonography is inconclusive or
additional structures are suspected. Early surgical intervention and
excision of Müllerian remnants are essential to reduce malignancy
risk and optimize long-term outcomes.
References
Citation
Jyoti N, Shraddha RS, Shrinivas BD, Ritu K, Chandresh K, et al.. Crossed Testicular Ectopia (CTE) Associated with Persistent Mullerian Duct Syndrome (PMDS): Case Report with Review of Literature. Indian J Appl Radiol. 2025;11(1): 220.