Case Report
Dominant Interarterial Ramus in a Right- Sinus Single Coronary Artery: A Case Report on Deviation from Lipton’s Classic R-III Variant on CT- CAG
Pushkar Mahajan, Chandresh Karnavat and Shrinivas B. Desai
1DNB Radiology Resident, Jaslok Hospital and Research Centre, Mumbai, India
2Consultant Radiologist, Jaslok Hospital and Research Centre, Mumbai, India
3Head of Radiology Department, Jaslok Hospital and Research Centre, Mumbai, India
2Consultant Radiologist, Jaslok Hospital and Research Centre, Mumbai, India
3Head of Radiology Department, Jaslok Hospital and Research Centre, Mumbai, India
*Corresponding author:Dr. Pushkar Mahajan, Department of Radiodiagnosis and Imaging Jaslok Hospital and Research Centre Mumbai, Maharashtra, India E-mail Id:mahajan.pushkar@icloud.com
Copyright: ©2025 Mahajan P, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information:Submission: 10/07/2025; Accepted: 05/08/2025; Published: 08/08/2025
Abstract
Single coronary artery (SCA) is a rare congenital coronary anomaly in which all three major coronary arteries arise from a single aortic sinus. We present a unique case of a 59-year-old female who underwent coronary computed tomography angiography (CTA) for evaluation of new-onset ventricular ectopics
and epigastric discomfort. Imaging revealed a solitary coronary artery arising from the right sinus of Valsalva, giving rise to the right coronary artery (RCA), left anterior descending artery (LAD), left circumflex artery (LCx), and a prominent ramus intermedius. The LAD had a benign prepulmonic course, while the
LCx followed a retroaortic route. Notably, the ramus intermedius coursed between the aorta and pulmonary artery (interarterial), and was the dominant vessel supplying the lateral wall of the left ventricle due to diminutive obtuse marginal branches. This configuration is a previously undescribed variant diverging from the classic R-III Lipton classification and represents a potentially malignant anomaly. Recognition of such atypical and hemodynamically significant variants is crucial for clinical risk stratification and interventional planning.
Keywords: Single Coronary Artery; Lipton Classification Variant; Interarterial Ramus; Coronary CT Angiography; Malignant Coronary Anomaly; R-III Deviation
Abbreviations
SCA – single coronary artery; R – right sinus of Valsalva; L – le
sinus of Valsalva; RCA – right coronary artery; LAD – le
anterior
descending artery; LCx – le
circum
ex artery; LMCA – le
main
coronary artery; RI – ramus intermedius; A – prepulmonic course
(anterior to pulmonary artery); B – interarterial course (between aorta
and pulmonary artery); P – retroaortic course (posterior to aorta).
Introduction
Coronary artery anomalies (CAAs) are rare congenital
abnormalities, occurring in less than 1% of the population undergoing
coronary angiography [1]. Among these, single coronary artery
(SCA) anomalies—where one coronary artery arises from a solitary
ostium—are particularly uncommon, with a reported prevalence
between 0.024% and 0.066% [2].
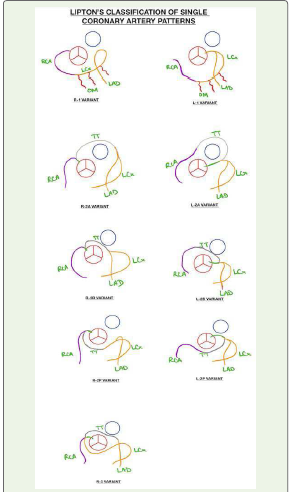
Lipton et al. classified SCAs based on the sinus of origin (right or
le
) and the anatomical distribution pattern of the coronary branches
[3]. This system is widely used to describe and stratify the potential
clinical relevance of various SCA subtypes.
The clinical significance of SCAs depends largely on the
course the vessels take. Benign variants may be asymptomatic and
discovered incidentally, whereas malignant variants, particularly
those with an interarterial course, may pose a risk for myocardial
ischemia or sudden cardiac death [4]. Our case presents an atypical
configuration with a malignant interarterial course of the ramus
intermedius, a variation that has not been explicitly described in the
Lipton classification system.
Case Report
A 59-year-old female with a history of new-onset ventriucular
ectopics and epigastric discomfort was referred for coronary CTA.
The scan was performed using ECG-gated multidetector CT a
er
administration of 100 ml of non-ionic contrast (Ultravist).
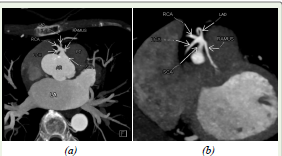
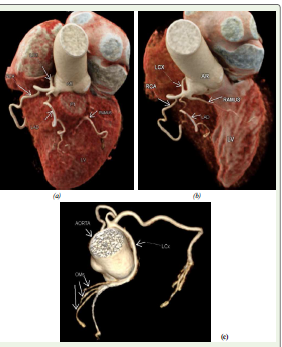
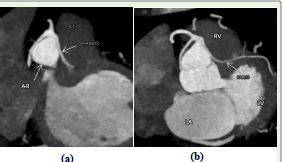
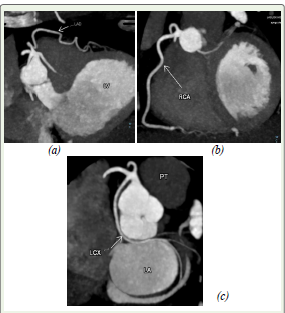
The study revealed a single coronary artery arising from the right sinus of Valsalva, bifurcating into four major branches: RCA, LAD, LCx, and a ramus intermedius.
• The LAD took a benign prepulmonic course anterior to the right ventricular out ow tract and terminated near the apex.
• The LCx had a retroaortic course, passing posterior to the aortic root and anterior to the atria, giving rise to narrow caliber obtuse marginal branches.
• The ramus intermedius, unusually dominant (obtuse marginal arteries and diagonal branches being very small in calibre), coursed between the aorta and pulmonary artery, representing an interarterial (malignant) course. It supplied the lateral wall of the le ventricle with no significant contribution from other lateral branches.
The study revealed a single coronary artery arising from the right sinus of Valsalva, bifurcating into four major branches: RCA, LAD, LCx, and a ramus intermedius.
• The LAD took a benign prepulmonic course anterior to the right ventricular out ow tract and terminated near the apex.
• The LCx had a retroaortic course, passing posterior to the aortic root and anterior to the atria, giving rise to narrow caliber obtuse marginal branches.
• The ramus intermedius, unusually dominant (obtuse marginal arteries and diagonal branches being very small in calibre), coursed between the aorta and pulmonary artery, representing an interarterial (malignant) course. It supplied the lateral wall of the le ventricle with no significant contribution from other lateral branches.
No coronary ostia were visualized in the le
or non-coronary
sinuses. The coronary arteries showed no significant atherosclerosis,
and calcium score was zero.
Discussion
SCA anomalies with origin from the right sinus are less common
than those from the le
. The R-III subtype, as seen in this case, is
among the rarest configurations described in Lipton’s classification,
where all major coronary arteries arise from the right sinus and follow
separate anomalous courses [3,5].
Lipton’s classification system categorizes SCAs using a
combination of origin site (“R” for right sinus, “L” for le
), and
further subclassies them into three types:
• Type I: A single coronary artery follows the course of either a normal right or le coronary artery.
• Type II: The single coronary artery bifurcates into right and le systems.
• Type III: The left anterior descending (LAD) and le circumflex (LCx) arteries arise separately from the proximal right coronary artery (RCA), as in our case.
• Type I: A single coronary artery follows the course of either a normal right or le coronary artery.
• Type II: The single coronary artery bifurcates into right and le systems.
• Type III: The left anterior descending (LAD) and le circumflex (LCx) arteries arise separately from the proximal right coronary artery (RCA), as in our case.
Each type is further classified based on the anatomic course
taken by the arteries: “A” for anterior to the pulmonary artery
(prepulmonic), “B” for between the aorta and pulmonary artery
(interarterial), and “P” for posterior to the aorta (retroaortic).
In our case, the LAD demonstrated a benign prepulmonic
course and the LCx had a retroaortic course. However, the ramus
intermedius presented a critical deviation—coursing interarterially in
a hemodynamically dominant fashion, with narrow obtuse marginals
failing to compensate. This raises concern for compression between
the great vessels, especially under stress conditions, posing a potential
risk for myocardial ischemia or sudden cardiac death [4,6].
To date, a dominant ramus intermedius with a malignant
interarterial course in the setting of a single coronary artery has
not been clearly documented in literature. A report by Paolillo et
al. described a ramus artery with an intraseptal course, potentially
subject to systolic compression, but without a truly interarterial
trajectory [8]. Another reported case from Radiopaedia involved a
trifurcating le
main artery with interarterial le
main and ramus
courses; however, that anatomy did not arise from a single coronary

ostium [9]. This highlights the uniqueness of our case as the first to
combine a single right sinus origin, dominant interarterial ramus, and
classic R-III branching anatomy with significant lateral wall supply.
Conclusion
We report a novel variant of a single coronary artery arising
from the right sinus of Valsalva with a malignant interarterial ramus
intermedius, a prepulmonic LAD, and retroaortic LCx. This deviates
from the classic R-III subtype of Lipton classification and warrants
attention due to the hemodynamic dominance and malignant course
of the ramus. Recognition and documentation of such variations are
essential for clinical decision-making and procedural safety.
Table 1: Summary of Lipton classification of single coronary artery (SCA) anomalies and comparison with previously reported anomalous coronary patterns.
The table outlines key features of each Lipton subtype (Types I–III), highlighting differences in origin, branching, course of the coronary arteries and compares it to our case.
Our case demonstrates a novel variation with a dominant ramus intermedius arising from a right sinus SCA and taking a malignant interarterial course, which has not been previously documented in literature.
Table 1: Summary of Lipton classification of single coronary artery (SCA) anomalies and comparison with previously reported anomalous coronary patterns.
The table outlines key features of each Lipton subtype (Types I–III), highlighting differences in origin, branching, course of the coronary arteries and compares it to our case.
Our case demonstrates a novel variation with a dominant ramus intermedius arising from a right sinus SCA and taking a malignant interarterial course, which has not been previously documented in literature.
References
Citation
Mahajan P, Karnavat C, Desai SB. Dominant Interarterial Ramus in a Right-Sinus Single Coronary Artery: A Case Report on Deviation from Lipton’s Classic R-III Variant on CT- CAG. Indian J Appl Radiol. 2025;11(1): 218.