Case Report
A Case Report of Spindle Cell Neoplasm (Leiomyoma) of Jejunum Presenting as Overt Lower Gastrointestinal Bleeding- A Radiological Perspective
Akhil. M. Kulkarni, Maheshwari M Pujari, Suhasini Vittal Rao and Srinivas S
1Consultant fetal medicine specialist, Davangere Scan centre, Karnataka, India.
2Department of Radiology SSIMS & RC Davangere, Karnataka, India.
3Consultant surgeon, Davangere, Karnataka, India.
2Department of Radiology SSIMS & RC Davangere, Karnataka, India.
3Consultant surgeon, Davangere, Karnataka, India.
*Corresponding author:Suhasini Vittal Rao, Consultant fetal medicine specialist, Davangere scan centre, Davangere, Karnataka, India, E-mail: drsuhasini2010@gmail.com
Copyright: © 2025 Kulkarni AM, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information:Submission: 16/06/2025; Accepted: 05/08/2025; Published: 06/08/2025
Abstract
Background: Diagnosing gastrointestinal (GI) bleeding using radiological methods remains challenging, particularly when conventional endoscopic and imaging techniques fail to reveal a clear source. Computed tomography (CT) plays a supportive role by helping to localize the bleeding and identify potential
causes, supplementing other modalities like endoscopy, nuclear scans, and angiography. This report emphasizes the diagnostic utility of multiphase contrast enhanced CT enterography in detecting a rare benign smooth muscle tumor —jejunal leiomyoma—as the source of GI bleeding.
Case Presentation: We present the case of a 50-year-old woman who experienced acute hematochezia. Both upper GI endoscopy and colonoscopy were inconclusive. Multiphase contrast-enhanced CT enterography, performed with neutral contrast, demonstrated a well-defined, enhancing extra luminal mass in the proximal jejunum. Surgical resection followed by histopathological analysis confirmed the mass as a spindle cell tumor, consistent with a leiomyoma.
Conclusion: This case highlights the value of multiphase CT enterography in pinpointing bleeding sources and characterizing bowel lesions, thereby guiding surgical decisions. It also brings attention to a rare manifestation of small bowel leiomyoma presenting with overt lower GI bleeding.
Case Presentation: We present the case of a 50-year-old woman who experienced acute hematochezia. Both upper GI endoscopy and colonoscopy were inconclusive. Multiphase contrast-enhanced CT enterography, performed with neutral contrast, demonstrated a well-defined, enhancing extra luminal mass in the proximal jejunum. Surgical resection followed by histopathological analysis confirmed the mass as a spindle cell tumor, consistent with a leiomyoma.
Conclusion: This case highlights the value of multiphase CT enterography in pinpointing bleeding sources and characterizing bowel lesions, thereby guiding surgical decisions. It also brings attention to a rare manifestation of small bowel leiomyoma presenting with overt lower GI bleeding.
Keywords: Lower gastrointestinal (GI) bleeding, Computed Tomography Enterography (CTE), Upper gastrointestinal (UGI) endoscopy.
Introduction
Lower gastrointestinal (GI) bleeding is defined as bleeding that
originates from the GI tract distal to the ligament of Treitz. While
upper GI bleeding is more frequently encountered in clinical practice,
bleeding from the lower GI tract remains an important and potentially
serious condition. Small bowel sources are responsible for roughly
5–10% of all GI bleeding cases [1].
Visible, or overt, GI bleeding-such as hematemesis, hematochezia,
or melena-can be life-threatening and often necessitates a
multidisciplinary approach to establish the diagnosis and guide
therapy.
To evaluate small bowel sources of bleeding, several diagnostic
methods are available. These include upper GI endoscopy,
colonoscopy, nuclear medicine scans, video capsule endoscopy, and
more recently, multiphase contrast-enhanced CT enterography.
Although extended endoscopic procedures may detect
abnormalities in about one-third of patients, their reach is limited
when it comes to the distal segments of the small intestine. Capsule
endoscopy has a variable sensitivity (ranging from 42% to 80%) in
detecting lesions within the small bowel responsible for GI bleeding
[2].
While nuclear medicine techniques are highly sensitive in
detecting bleeding, their ability to precisely localize the site is limited
due to relatively poor spatial resolution and insufficient anatomical
detail. These scans also require significant time, specialized personnel,
and equipment, which can limit their availability in acute settings [3].
Video capsule endoscopy, widely used in cases of obscure or
intermittent GI bleeding, allows direct visualization of the small
bowel mucosa. However, its utility in emergent situations remains
uncertain [3].
Multiphase contrast-enhanced CT enterography has emerged as
a valuable imaging modality for evaluating small bowel pathology.
This technique combines the use of a multi-detector CT scanner with
luminal distension achieved through the administration of a neutral
oral contrast agent. Images are acquired in multiple phases—precontrast,
late arterial, portal, and venous—following intravenous
contrast administration. This cross-sectional method helps localize
the bleeding site and identify underlying causes.
The high-resolution imaging and the ability to detect both
bowel wall and extra-intestinal abnormalities have positioned CT
enterography as a crucial tool in assessing small bowel disease.
Leiomyomas of the gastrointestinal (GI) tract are uncommon
accounting for less than 1–2% of all benign small bowel tumours.
Among small bowel neoplasms, spindle cell tumors are often
gastrointestinal stromal tumors (GISTs), while leiomyomas represent
a rare benign subset. They typically arise from the muscularis
propria and grow extraluminally, often remaining asymptomatic
until they reach a size that causes obstruction, intussusception, or
vague abdominal discomfort. Bleeding, particularly overt lower
gastrointestinal bleeding, is an uncommon presentation and is
more frequently associated with mucosal ulceration overlying the
tumor surface. This rarity, combined with the nonspecific nature of
symptoms, contributes to frequent delays in diagnosis.
This case report describes a rare presentation of a proximal jejunal
small leiomyoma in a 50-year-old female, with overt lower GI bleed as
the initial clinical manifestation, emphasizing radiologic evaluation
and its diagnostic value.
Case description
A 50-year-old female reported with a five-day history of bright
red rectal bleeding (hematochezia), which was sudden in onset and
not associated with abdominal pain or altered bowel habits. She
also experienced progressive fatigue and light-headedness over this
period. There was no history of NSAID use, anticoagulant therapy, or
prior gastrointestinal symptoms.
On initial assessment, her vital signs were stable, and abdominal
examination revealed no abnormalities.
Initial laboratory investigations revealed mild anemia with hemoglobin of 9 g/dL, hematocrit of 28%, and a normal platelet count. Coagulation parameters, including PT/INR and aPTT, were within normal limits. Renal and liver function tests were unremarkable.
Initial laboratory investigations revealed mild anemia with hemoglobin of 9 g/dL, hematocrit of 28%, and a normal platelet count. Coagulation parameters, including PT/INR and aPTT, were within normal limits. Renal and liver function tests were unremarkable.
An upper gastrointestinal endoscopy was performed but yielded
no findings. Similarly, colonoscopy failed to detect any source of
bleeding within the visualized segments.

Discussion
Multiphase Contrast-Enhanced CT Enterography:
The main objective of CT imaging in cases of suspected GI
bleeding is to detect the presence of blood within the intestinal lumen,
observe contrast extravasation, and identify the underlying cause of
bleeding.Imaging Equipment and Technical Parameters: Multiphase contrast-enhanced CT enterography was performed using a 128-slice multidetector CT scanner (REVOLUTION EVO, Wipro GE). The following parameters were used:
• Tube voltage: 120 kVp
• Tube current: 200 mAs (effective)
• Rotation time: 0.35 seconds
• Collimation: 0.5 mm slice thickness
• Pitch: 1.375:1 • Reconstruction interval: 1 mm
• Tube current: 200 mAs (effective)
• Rotation time: 0.35 seconds
• Collimation: 0.5 mm slice thickness
• Pitch: 1.375:1 • Reconstruction interval: 1 mm
Protocol:
After a fasting period of 4–6 hours, the patient ingested
approximately 1500 mL of neutral oral contrast solution (such as isoosmotic
mannitol) over a span of 40-60 minutes. This neutral contrast
is essential for optimal bowel wall visualization, as it enhances the
contrast between the bowel lumen and its enhancing mucosa,
improving the detection of pathology.Multiphase imaging was conducted following administration of intravenous contrast and the use of an antispasmodic agent (e.g., visceralgine or Buscopan, 0.5 mg IV) to reduce bowel motility and improve image clarity. A non-contrast scan of the abdomen was followed by contrast-enhanced scans during the arterial, portal, and venous phases. Intravenous contrast (120 mL of nonionic contrast at 350 mg/mL) was injected at a rate of 4 mL/s. Image data were then processed for multiplanar reconstruction on a dedicated workstation.
Radiological Interpretation:
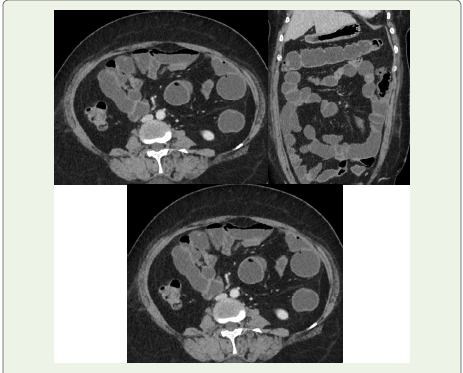
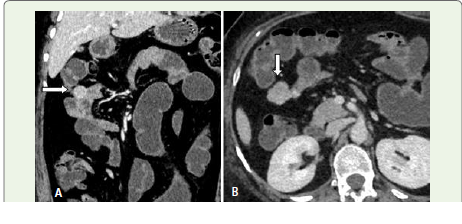
Findings on CT Enterography: CT enterography &
angiography of the abdomen and pelvis revealed a ~ 27 x 20 mm
well-circumscribed, extra-luminal enhancing lesion in the proximal
jejunum (approximately 10 cm distal to the duodenojejunal
junction). The lesion demonstrated homogeneous enhancement with
a subtle intraluminal blush in arterial phase. No signs of obstruction
or adjacent invasion were observed.Jejunal leiomyomas generally arise from the muscular layers—
typically the muscularis propria—and may extend outward. They may
erode the mucosa, leading to bleeding. Radiologically, they appear
as smooth, enhancing, well-defined lesions. In cases of mucosal
ulceration, active bleeding may be visualized as contrast extravasation
on angiographic phases.
Surgical and Histopathological Findings: The patient underwent
an exploratory laparotomy, during which a segmental resection of
the affected jejunal portion was performed. Intra-operatively, a well encapsulated
extraluminal mass was observed protruding from the
jejunal wall. The overlying mucosa was congested and showed areas
of ulceration, correlating with the site of bleeding.
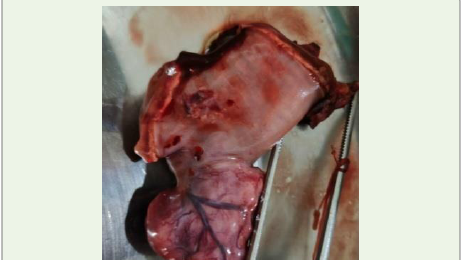
Gross pathology:Examination of the resected specimen revealed
a firm, well-demarcated mass arising from the jejunal wall and
extending outward beyond the lumen. The mucosal surface overlying
the mass was disrupted, and several dilated blood vessels were noted
in the surrounding area.
Histological analysis demonstrated that the lesion originated
from the muscularis propria. It was composed of spindle-shaped
cells arranged in characteristic interlacing fascicles. The individual
cells featured elongated nuclei and moderate amounts of eosinophilic
cytoplasm. No signs of atypia, increased mitotic activity, or necrosis
were observed. Numerous dilated and congested blood vessels were
also identified within the lesion.
These findings confirmed the diagnosis of a benign spindle cell tumor of smooth muscle origin—specifically, a leiomyoma. While gastrointestinal stromal tumors (GISTs) represent the more common spindle cell tumors in the small bowel, this lesion lacked the immune histochemical and morphological features typical of GISTs. The absence of malignant characteristics further supported the diagnosis of leiomyoma.
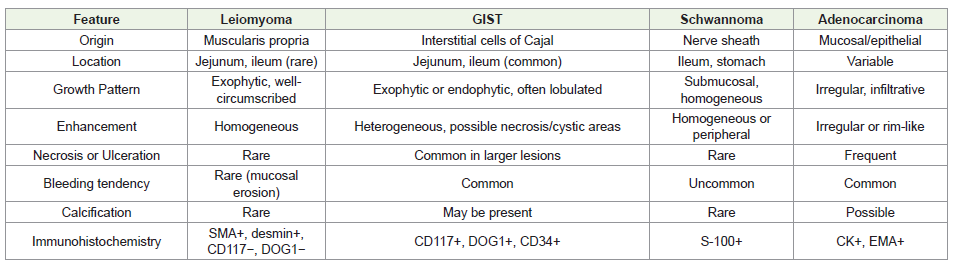
Spindle Cell Tumors of The Small Bowel: Spindle cell tumors of the small bowel represent a heterogeneous group of lesions, and accurate diagnosis often requires correlation between imaging, histopathology, and immunohistochemistry. The key differentials include:
These findings confirmed the diagnosis of a benign spindle cell tumor of smooth muscle origin—specifically, a leiomyoma. While gastrointestinal stromal tumors (GISTs) represent the more common spindle cell tumors in the small bowel, this lesion lacked the immune histochemical and morphological features typical of GISTs. The absence of malignant characteristics further supported the diagnosis of leiomyoma.
Spindle Cell Tumors of The Small Bowel: Spindle cell tumors of the small bowel represent a heterogeneous group of lesions, and accurate diagnosis often requires correlation between imaging, histopathology, and immunohistochemistry. The key differentials include:
− Gastrointestinal Stromal Tumors (GISTs)
− Leiomyomas
− Leiomyosarcomas
− Schwannomas
− Inflammatory Fibroid Polyps
− Desmoid Tumors
− Leiomyomas
− Leiomyosarcomas
− Schwannomas
− Inflammatory Fibroid Polyps
− Desmoid Tumors
Conclusion
This case highlights an unusual presentation of a proximal jejunal
leiomyoma manifesting as overt lower gastrointestinal bleeding.
It underscores the vital role of multiphase contrast-enhanced
CT enterography in the evaluation of small bowel pathology,
particularly in accurately localizing the bleeding source and aiding
in surgical planning. Although CT enterography provides highresolution
imaging capable of detecting intramural and extraluminal
abnormalities, superficial mucosal lesions and vascular anomalies
may still be missed, which remains a limitation [2].
Radiologists should remain vigilant for rare benign entities such as leiomyomas when interpreting enhancing spindle cell lesions of the small intestine. A multidisciplinary approach—integrating imaging, surgical findings, and histopathological confirmation—is essential for definitive diagnosis and appropriate management.
Radiologists should remain vigilant for rare benign entities such as leiomyomas when interpreting enhancing spindle cell lesions of the small intestine. A multidisciplinary approach—integrating imaging, surgical findings, and histopathological confirmation—is essential for definitive diagnosis and appropriate management.
Key Learning Points:
Rare Etiology: Proximal jejunal leiomyomas are an uncommon
but important differential in patients presenting with overt GI
bleeding.Imaging Utility: Multiphase contrast-enhanced CT enterography is a highly effective non-invasive tool for detecting and localizing sources of small bowel bleeding.
Histological Confirmation: Final diagnosis relies on histopathological evaluation and, when necessary, immuno histochemistry to differentiate leiomyoma from GIST and other spindle cell neoplasms.
Patient consent for publication was not obtained; however, this report contains no identifiable personal information, images, or data that could lead to patient identification. The case has been reported in full compliance with institutional and ethical guidelines.
References
Citation
Kulkarni AM, Pujari MM, Rao SV, Srinivas S. A Case Report of Spindle Cell Neoplasm (Leiomyoma) of Jejunum Presenting as Overt Lower Gastrointestinal Bleeding- A Radiological Perspective. Indian J Appl Radiol. 2025;11(1): 215.