Case Series
A Case Series in Evaluating Anomalous Coronary Artery Origins in Adults with 128-Slice-MDCT; Unmasking the Hidden Treats
Akhil. M. Kulkarni, Kewin Raj J and Suhasini Vittal Rao
1Consultant fetal medicine specialist, Davangere Scan center, Karnataka, India.
2Department of Radiology, SSIMS & RC, Davangere, Karnataka, India.
2Department of Radiology, SSIMS & RC, Davangere, Karnataka, India.
*Corresponding author:Suhasini Vittal Rao, Consultant fetal medicine specialist, Davangere Scan center, Karnataka, India. E-mail Id: drsuhasini2010@gmail.com
Copyright: © 2025 Kulkarni AM, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information:Submission: 16/06/2025; Accepted: 02/08/2025; Published: 05/08/2025
Abstract
Anomalies in the origin of coronary arteries (AOCA) though rare can lead to serious clinical outcomes such as myocardial ischemia or even sudden death. MDCT has transformed noninvasive evaluation of the coronary arteries by providing high-resolution imaging capabilities. Here is a case series of overview of the imaging features, classification, and clinical implications of anomalous coronary origins as seen on 128-slice MDCT, emphasizing its critical role in diagnosis, evaluating risk, and guiding surgical management. In our institute, a total of 250 MDCT coronary angiograms have been done over a period
of 2 years, after taking informed consents from the patients. Among them 5 cases had anomalies in the origin of coronary arteries (AOCA)—two cases of anomalous origin of RCA from left coronary sinus with malignant inter-arterial course, one with anomalous origin of Left main coronary artery from noncoronary
cusp with retro-aortic course, one with anomalous origin of Left circumflex artery from the right coronary sinus with malignant inter-arterial course and one case of separate origins of Left anterior descending artery and Left circumflex artery from left coronary sinus. Identification of benign and malignant
courses is also of utmost importance, because the later may warrant surgical intervention. In our case series the incidence rate of anomalous origins is 2%, closely aligning with those of existing studies in the literature.
Introduction
AOCA refers to a group of congenital coronary anomalies that
may be clinically silent or present with severe and potentially fatal
consequences. The growing use of MDCT has markedly enhanced the
identification and detailed assessment of these coronary variants [1,2]. Conventional coronary angiography has historically been the gold
standard for evaluating coronary anatomy, but it has limitations in
delineating the exact origin and 3D course of anomalous coronary
arteries, especially in relation to surrounding structures [3]. In recent
years, 128-slice MDCT or higher scanners, has emerged as a valuable
noninvasive imaging modality o
ering excellent spatial and temporal
resolution [4]. MDCT provides detailed anatomical information
regarding the origin, course and potential compression points of
anomalous vessels, which is important for both risk stratification and
surgical planning [7]. This review aims to outline the various AOCA
observed on 128-slice MDCT. These coronary anomalies are believed
to result from developmental errors in the embryonic formation of
coronary buds and their attachment to the aortic sinuses. AOCA
occurs in about 0.3% to 2% of individuals, and certain types are
associated with elevated risks, especially during physical activity in
younger patients [2,5].
Classification of Anomalous origin of coronary arteries:
AOCA can be classified into the following categories:
1. Anomalous aortic origin with normal course.2. Anomalous aortic origin with anomalous proximal course.
3. Anomalous origin from the pulmonary artery.
4. Single coronary artery.
These categories display unique imaging characteristics and clinical significance, & certain anomalies may necessitate operative management [6]
Classification of AOCA by Anatomic course and clinical risk:
[2,5,6]
LCX-Left circumflex artery; RCA- Right coronary artery; LCA-Left coronary artery;
Imaging Technique:
128-MDCT scanners o
er superior spatial detail, synchronized
ECG acquisition, and 3D image reconstruction [1]. Beta-blockers and
sublingual nitroglycerin are commonly administered before scanning
to enhance image quality. High-resolution thin-section imaging,
curved multiplanar reconstructions and 3D volume-rendered views
are essential for assessing the origin, trajectory and ostial details of
coronary vessels [5,7].Case Illustrations:
Case 1: A 70-year-old female with c/o dyspnea on exertion, case
of hypertension and diabetes mellitus, demonstrated an anomalous
origin of Right coronary artery from le
coronary sinus, RCA seen
passing between the pulmonary trunk & ascending aorta– Malignant
inter-arterial course of RCA.Case 2: A 36-year-old male smoker with c/o chest pain & positive stress test and without any comorbidities, demonstrated an anomalous origin of Le main coronary artery from non-coronary cusp with retro-aortic course.
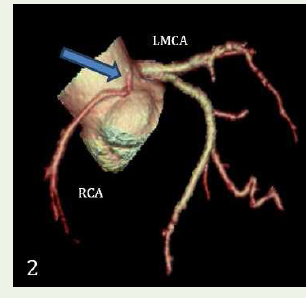
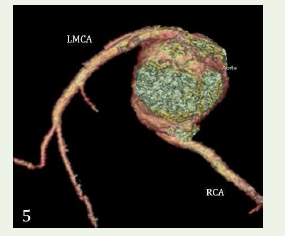
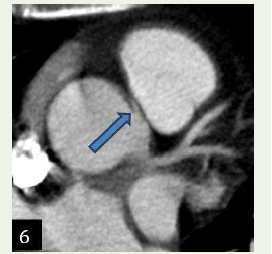
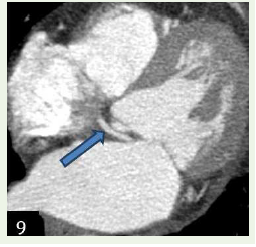
Case 3: A 45-year-old male smoker & alcoholic with c/o chest discomfort & mildly positive stress test demonstrated an anomalous origin of Right coronary artery from the le coronary sinus with malignant inter-arterial course.
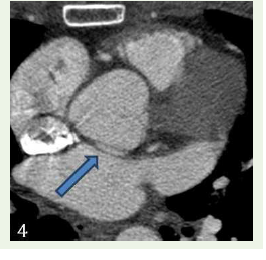
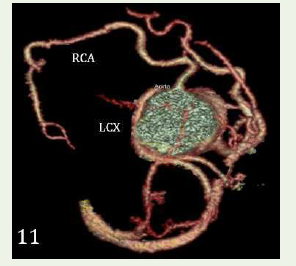
Case 4: A 68-year-old female with c/o chest pain, case of hypercholesterolemia and diabetes and concentric le ventricular hypertrophy in echocardiogram, demonstrated an anomalous origin of Left circumflex artery from the right coronary sinus with retro- aortic course.
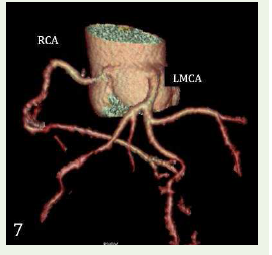
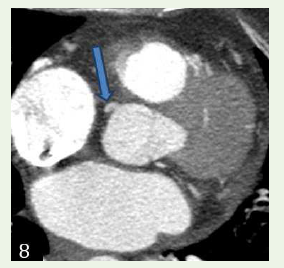
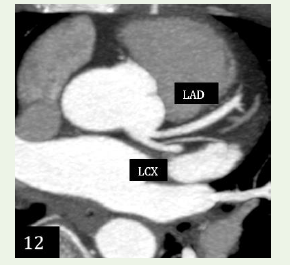
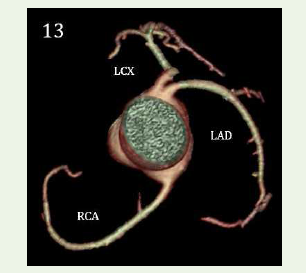
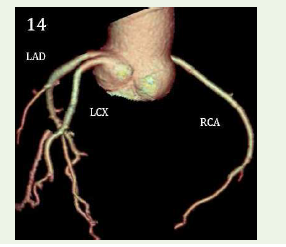
Case 5: A 48-year-old female with chest pain for 2 days, normal echocardiography, mildly positive for inducible ischemia in TMT with hypercholesterolemia demonstrated an anomalous separate origin of Left anterior descending and left circum ex artery from left coronary sinus.
Clinical Significance and Management:
Low-risk anomalies like retroaortic or prepulmonic routes are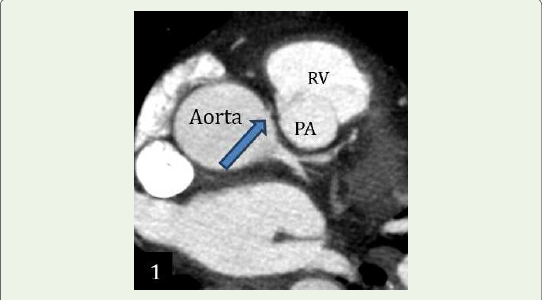


usually treated with observation alone. Serious anomalies such as
interarterial courses of the LMCA or RCA o
en require surgical
treatment—like unroofing or reimplantation—making precise
imaging and reporting crucial for preoperative strategy [4,5]. All
the AOCA cases in our series are managed conservatively with
observation.
Discussion
MDCT coronary angiography has emerged as the imaging modality
of choice for delineating coronary anomalies owing to its high spatial
resolution, non-invasiveness and ability to generate multiplanar and
three-dimensional reconstructions. Our findings demonstrate that
128-slice MDCT reliably detected the origin & course of anomalous
coronary arteries, including high-risk variants such as an inter-arterial
course (between the aorta and pulmonary artery), which has been
associated with sudden cardiac events. In contrast to conventional
catheter angiography, MDCT provides superior visualization of the
proximal vessel origin and its relationship with adjacent structures,
which is o
en crucial for surgical or interventional planning [8]
Familiarity with the CT imaging features of coronary anomalies
and their clinical relevance is vital for correct diagnosis and effective
patient management [5]. While many coronary anomalies are
harmless, those that travel between the major vessels pose a risk
for ischemia and sudden cardiac death. the rising use of MDCT
in cardiac imaging underscores the importance of detecting these
anomalies through axial, multiplanar and 3D reconstructions [1].
AOCA cases in our series didn’t undergo any surgical management
but were managed conservatively with observation. Our studies
underlines the indispensable role of 128-slice MDCT in the modern
diagnostic approach to anomalous origin of coronary arteries.
References
Citation
Kulkarni AM, Raj JK, Rao SV. A Case Series in Evaluating Anomalous Coronary Artery Origins in Adults with 128-Slice-MDCT; Unmasking the Hidden Threats. Indian J Appl Radiol. 2025;11(1): 214.