Pictorial Review Article
Bowel Anastomotic Leaks: A Pictorial Review of Salient Findings on Computed Tomography (CT)
Shipra Kumari1*, Pallavi Rao2 and Arjun Kalyanpur3
1Consultant Radiologist, Teleradiology Solutions, Whitefield, Bangalore, India
2Senior Scientific Officer, Image Core Lab, Whitefield, Bangalore, India
3Chief Radiologist, Teleradiology Solutions, Whitefield, Bangalore, India
2Senior Scientific Officer, Image Core Lab, Whitefield, Bangalore, India
3Chief Radiologist, Teleradiology Solutions, Whitefield, Bangalore, India
*Corresponding author:Shipra Kumari, Consultant Radiologist, Teleradiology Solutions, Whitefield, Bangalore, India Email:shipra.kumari@telradsol.com
Copyright: © 2025 Kumari S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information:Submission: 01/04/2025; Accepted: 15/05/2025; Published: 20/05/2025
Abstract
Background: Anastomotic leaks can occur in early and late post-operative phase when enteric anastomosis fails. Undiagnosed anastomotic leak carries a poor outcome. Therefore, knowledge of accurate interpretation of CT imaging characteristics is vital for a timely and accurate diagnosis of anastomotic leak.
Aims and objectives: The purpose of this study is to assess the salient imaging findings of bowel anastomotic leak on Computed Tomography and compile a pictorial review useful in the identification of anastomotic leaks after gastrointestinal tract surgery.
Materials and Methods: We retrospectively evaluated 49 CT abdomen and pelvis studies which were diagnosed to have post-surgical anastomotic leak as based on keyword search from Emergency Teleradiology reports. Out of 49 cases, non-contrast (17), IV contrast (17), oral contrast (4), oral and IV contrast (10) and rectal contrast (1) were identified. The results were analysed and compiled in a pictorial review. Results: Our study demonstrated that extraluminal air was the most common imaging finding seen in14.21% of patients. Focal collection or abscess (13.7%), peritonitis in (12.3%), bowel wall thickening (5.4%) and intra-abdominal free fluid (2.9%) of examinations. Few other imaging findings included entero-cutaneous fistula in 2% of the cases and bowel obstruction in one case.Out of 14 examinations performed after administration of enteric contrast, 10 cases were positive for extravasation of intra-luminal contrast.
Conclusion: Early intervention in patients with anastomotic leak has shown to improve the ultimate outcome, especially with respect to mortality. Abdominal CT is a highly accurate non-invasive test in the detection of anastomotic leak.
Aims and objectives: The purpose of this study is to assess the salient imaging findings of bowel anastomotic leak on Computed Tomography and compile a pictorial review useful in the identification of anastomotic leaks after gastrointestinal tract surgery.
Materials and Methods: We retrospectively evaluated 49 CT abdomen and pelvis studies which were diagnosed to have post-surgical anastomotic leak as based on keyword search from Emergency Teleradiology reports. Out of 49 cases, non-contrast (17), IV contrast (17), oral contrast (4), oral and IV contrast (10) and rectal contrast (1) were identified. The results were analysed and compiled in a pictorial review. Results: Our study demonstrated that extraluminal air was the most common imaging finding seen in14.21% of patients. Focal collection or abscess (13.7%), peritonitis in (12.3%), bowel wall thickening (5.4%) and intra-abdominal free fluid (2.9%) of examinations. Few other imaging findings included entero-cutaneous fistula in 2% of the cases and bowel obstruction in one case.Out of 14 examinations performed after administration of enteric contrast, 10 cases were positive for extravasation of intra-luminal contrast.
Conclusion: Early intervention in patients with anastomotic leak has shown to improve the ultimate outcome, especially with respect to mortality. Abdominal CT is a highly accurate non-invasive test in the detection of anastomotic leak.
Keywords:Anastomotic Leak; Peritonitis; Free Fluid; Bowel Wall Thickening
Introduction
Anastomotic leaks are one of the most serious post-operative
complications that can occur after a bowel surgery [1]. Anastomotic
leaks can occur in early and late post-operative phases when
enteric anastomosis fails [2]. The International Study Group of
Rectal Cancer (ISREC) proposed a definition and grading system for
colorectal anastomotic leaks in 2010. The ISREC defined a leak as “a
defect of the intestinal wall at the anastomotic site (including suture
and staple lines of ano-rectal reservoirs) leading to a communication
between the intra- and extraluminal compartments.”[3]. The ISREC
delineated leaks by grades A to C based on their clinical management
which have been validated [4].
Anastomotic leaks following bowel surgery can be classified
into various categories, distinguishing between simple fistulas
and large sinuses, as well as intra-peritoneal and extra-peritoneal
occurrences. These leaks may exhibit sepsis-producing symptoms
or remain asymptomatic, and their timing can be either early or late
post-operative period [5]. Detecting an anastomotic leak relies on
clinical suspicion and subsequent diagnostic investigations. When
located within the peritoneal cavity, leaks are more likely to manifest
with diffuse contamination, peritonitis, and sepsis. On the other
hand, extra-peritoneal leaks may present in a less obvious manner,
possibly appearing as a fistula, rectal drainage, pain, or even urinary
symptoms. Understanding the diverse manifestations of anastomotic
leaks is crucial for the timely and accurate management of this
serious post-operative complication [6,7]. The most consistent and
significant risk factor for an anastomotic leak is the anatomic site
of anastomosis [8]. The risk is higher with distal anastomotic sites.
An ileocolic anastomosis has a leak rate of 1-4% as compared to
colorectal anastomosis which carries a risk of 0.5-18% and coloanal
anastomosis which carries a risk of 5-19% [9]. Undiagnosed
anastomotic leak carries a poor outcome. Therefore, knowledge of
accurate interpretation of CT imaging characteristics is vital for a
timely and accurate diagnosis of anastomotic leak [10].
Aims and objectives
• To assess the salient imaging findings of bowel anastomotic
leak on CT.
• To compile a pictorial review useful in the identification of anastomotic leaks after gastrointestinal tract surgery.
• To compile a pictorial review useful in the identification of anastomotic leaks after gastrointestinal tract surgery.
Materials and Methods
We retrospectively evaluated 49 CT abdomen and pelvis studies
which were diagnosed to have post-surgical anastomotic leak based
on keyword search from Emergency Teleradiology reports. Images
were assessed for salient imaging findings of bowel anastomotic leak.
The results were analysed and compiled in a pictorial review.
Results
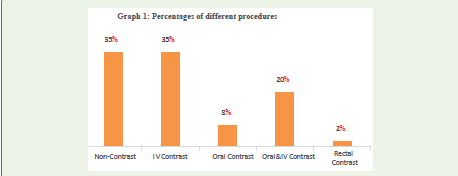
Out of the 49 CT abdomen and pelvis studies, 17 cases where noncontrast
and 32 cases were with contrast. Further out of 32 contrast
CT cases, 17 cases were IV contrast, 4 cases were oral contrast, and 10
cases were oral and IV contrast and 1 case with rectal contrast. Our
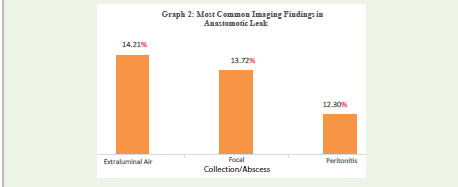
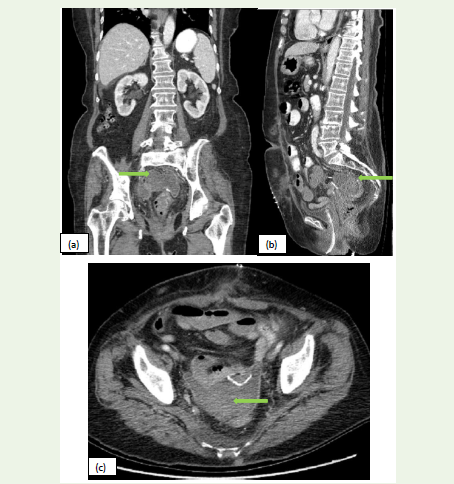
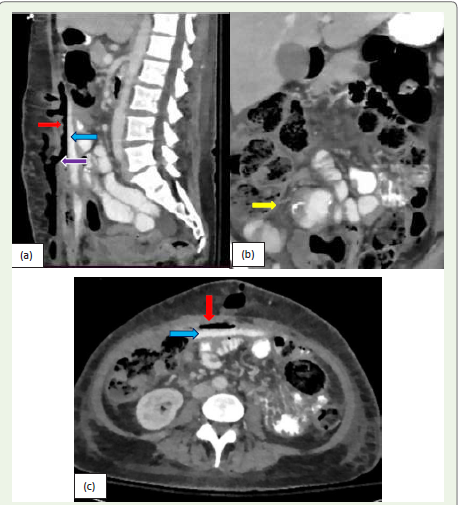
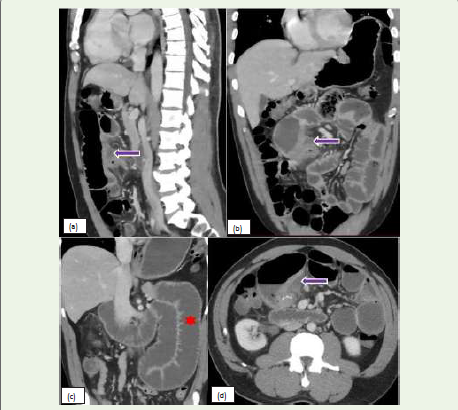
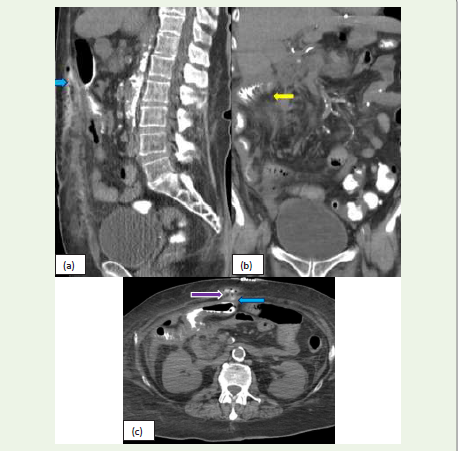
study demonstrated that extra-luminal air was the most common
imaging finding seen in 14.21% of patients. Other common findings
include focal collection or abscess (13.7%), peritonitis (12.3%). Few
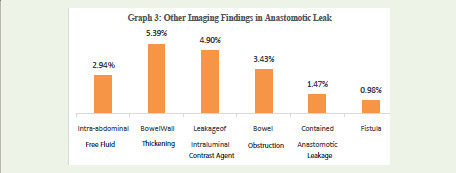
other uncommon imaging findings includes bowel wall thickening
(5.4%), intra-abdominal free fluid (2.9%), and extravasation of
intra-luminal contrast (4.9%), bowel obstruction (3.43), contained
anastomotic leak (1.47%) and fistula (0.98%).
Discussion
The most important role of imaging patients with suspected

anastomotic leaks is to rule out if a leak exists. This helps in patient
management including the need for repeat surgery versus watchful
waiting. Hence, it is very important to determine the imaging
findings that are most helpful in making an accurate diagnosis [1].
This pictorial review demonstrates findings helpful in making the
diagnosis of an extraluminal air amount and fluid collection density
anastomotic leak.
Extraluminal air was one of the most common findings seen
on CT images. Anastomotic leaks with abscess formation were the
second most common imaging finding, and studies show that it is
mostly seen in patients with Crohn’s disease [11]. The amount of
extra-luminal air and density of fluid collection has no prognostic
value wherein predicting an anastomotic leak [12]. Peritonitis was
another most-seen imaging finding. In cases of free/generalized
leak, there is complete dehiscence causing diffuse peritonitis due to
contamination of the abdomen by bowel contents. In cases of the
contained leak, there is limited contamination of the abdominal cavity
with localized peritonitis. Free leakage can present with abdominal
pain, fever, leucocytosis, hypotension, and altered mental state [13].
However, clinical features of contained leakage are non-specific, e.g.
intestinal obstruction, fistulas, and pelvis abscess near anastomosis
[14]. Contrast medium at the site of anastomosis is very important in
detecting anastomotic leaks after colorectal surgeries [15].
Conclusion
Anastomotic leak remains the main cause of morbidity and
mortality after colorectal surgeries, and hence timely diagnosis and
adequate treatment are important. Abdominal CT has become the
method of choice for assessing anastomotic leaks. Identification of
the most common CT findings helps in early detection in the early
postoperative phase.
References
Citation
Kumari S, Rao P, Kalyanpur A. Bowel Anastomotic Leaks: A Pictorial Review of Salient Findings on Computed Tomography (CT). Indian J Appl Radiol. 2025;11(1): 213.