Case Report
Rare Coexistence of Left Ventricular and Pericardial Hydatid Cysts: A Multimodal Imaging Case
Bharti AS, Kumar A, Shreya, and Jahan A*
Department of Radiodiagnosis, Moti Lal Nehru Medical College, Prayagraj, Uttar Pradesh, India
*Corresponding author:Arjumand Jahan, Department of Radiodiagnosis, Moti Lal Nehru Medical College, Prayagraj, Uttar Pradesh, India. E-mail Id: jahan.arjumand@gmail.com
Copyright: © 2025 Bharti AS, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information:Submission: 21/03/2025; Accepted: 28/04/2025; Published: 05/05/2025
Abstract
Intracardiac hydatidosis is a rare but potentially fatal manifestation of Echinococcus granulosus infection. Left ventricular involvement is the most common cardiac site, but pericardial involvement is unusual. We report a rare case of a 45-year-old male with left ventricular and pericardial hydatidosis, who
came to the department of radiodiagnosis of Moti Lal Nehru Medical College, Prayagraj for cardiac CT with coronary angiogram, with complaints of chest pain and exertional dyspnoea. Imaging revealed two multiloculated cystic lesions, one each in the left ventricular myocardium and pericardium, respectively.
Introduction
Hydatid disease, also known as echinococcosis or hydatidosis,
is a parasitic infection caused by the larval stage of tapeworms of
the genus Echinococcus. The two most common species that cause
disease in humans are Echinococcus granulosus and Echinococcus
multilocularis. The liver is affected in approximately 60-80% of
cases, while the lungs are involved in 20-30% of cases [1,2]. Cardiac
involvement is rare with an incidence of 0.5%–2% in systemic
hydatidosis cases[3-5], due to the strong myocardial contractility and
continuous coronary circulation, which prevent cyst implantation.
When cardiac hydatidosis occurs, the left ventricle is the most
frequently affected site (due to its rich supply), followed by right
ventricle, pericardium, pulmonary artery, left atrial appendage, and
interventricular septum [6]. Pericardial involvement is even rarer
but can lead to serious complications such as pericardial effusion,
tamponade or constrictive pericarditis. We report a rare case of
left ventricular and pericardial hydatid cysts, diagnosed through
multimodal imaging.
Clinical History
A 45-year-old male, an egg vendor by occupation, presented with
complaints of chest pain and progressive exertional dyspnoea for
three months with no history of fever or weight loss.
The patient hails from a rural area with frequent exposure to livestock, including cattle and dogs, known intermediate and definitive hosts of Echinococcus granulosus. His occupation as an egg vendor often brought him into direct contact with potentially contaminated environments, increasing the risk for parasitic exposure. The region is known for endemic echinococcosis [8], which further supported clinical suspicion.
The patient hails from a rural area with frequent exposure to livestock, including cattle and dogs, known intermediate and definitive hosts of Echinococcus granulosus. His occupation as an egg vendor often brought him into direct contact with potentially contaminated environments, increasing the risk for parasitic exposure. The region is known for endemic echinococcosis [8], which further supported clinical suspicion.
Clinical Examination:
• Vital signs: PR: 96 bpm, BP: 110/65 mmHg, SpO₂: 98%.• Cardiovascular: mild tachycardia, normal heart sounds, no murmurs.
• Respiratory: Normal breath sounds.
Investigations:
Blood Tests:• Mild eosinophilia (Absolute Eosinophilic Count: 550 cells/ cu.mm.)
• Normal liver and renal function tests.
Imaging::
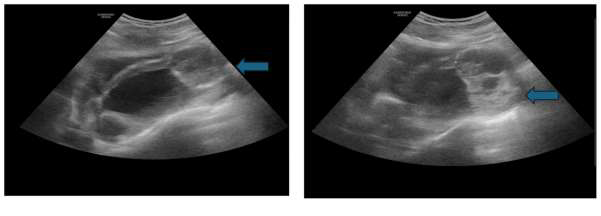
• 2D Echocardiography revealed a well-defined, multiloculated
cystic lesion in the left ventricular wall showing peripheral
calcifications, with no intracavitary obstruction [Figure 1a]
and another similar cystic lesion within the pericardial cavity,
adjacent to the left ventricle, without any signs of tamponade
[Figure 1b]. No significant hemodynamic obstruction noted.• Chest X-ray revealed a well-defined lobulated left paracardiac radioopacity. No other abnormal intrapulmonary opacity seen[Figure 2].
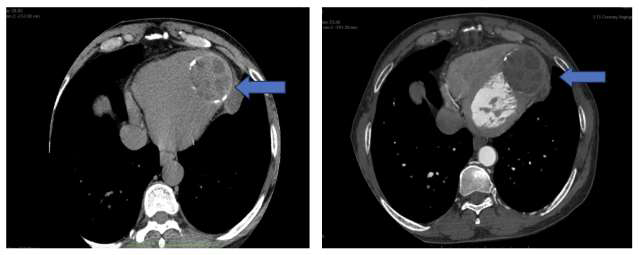
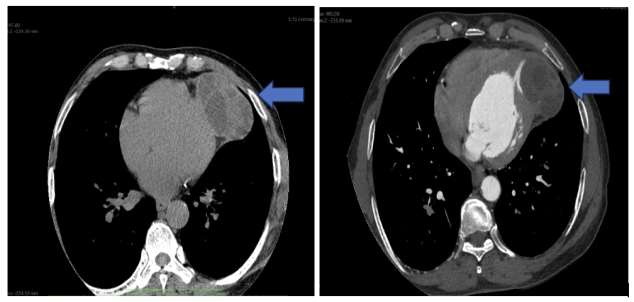
• Non-contrast and Contrast-enhanced Cardiac CT with Coronary angiography revealed A non-enhancing, welldefined, multiloculated cystic lesion with peripheral calcification within the mid-lateral wall of left ventricular myocardium [Figure 3a,3b]. Another multiloculated cystic lesion was noted in the left lateral pericardium adjacent to the left ventricular wall, suggestive of pericardial involvement [Figure 4a, 4b].
• Cardiac MRI: T2-weighted images revealed hyperintense cystic lesions in the left ventricle and pericardium.No significant pericardial effusion or thickening noted [Figure 5a,5b].


Diagnosis:
Based on multimodal imaging and blood tests, the patient was
diagnosed with intracardiac hydatidosis involving the left ventricular
myocardium and the pericardium.Management:
The patient was initiated on Albendazole at a dose of 15 mg/kg/
day, divided into two doses (400mg each), with meals. Treatment was
planned for at least 3months, with periodic liver function monitoring
and complete blood counts. The patient tolerated the initial course
well and was advised to continue under close outpatient follow-up.The patient was referred to a cardiothoracic surgical unit at
a higher centre for further evaluation. However, due to financial
constraints, he initially deferred surgery and opted for continued
medical management. At the last follow-up (3 months postdiagnosis),
the patient reported symptomatic improvement. A repeat
echocardiogram showed no significant change in cyst size or cardiac
function. Surgical excision remains under consideration pending
affordability and logistic support.
Diagnostic Considerations:
• Echocardiography is the first-line investigation.• CT provides detailed information on cardiac anatomy,
cyst walls and calcifications, and is excellent for detecting complications such as cyst rupture and pericardial effusion.
It can also be used for preoperative planning • MRI provides detailed anatomical information with superior soft tissue contrast and differentiates hydatid cysts from cardiac tumours.
• Serology confirms echinococcal infection but has variable sensitivity.
Discussion:
While cardiac hydatidosis itself is uncommon, simultaneous
involvement of both the left ventricle and pericardium is exceedingly
rare, with only isolated cases reported in literature [3-7]. This dualsite
presentation adds significant novelty to the present case and
underscores the importance of multimodal imaging in capturing
such atypical distributions.Cardiac hydatidosis is a diagnostic challenge due to its non-specific
symptoms [3,7]. The left ventricle, being highly perfused, is the most
common site, while pericardial involvement is rare [5]. Pericardial
hydatidosis may occur due to cyst rupture or hematogenous
spread [4]. A multimodal imaging approach, especially involving
echocardiography, CT, and MRI, is essential for diagnosis.
Echocardiographic Findings:
Transthoracic echocardiography (TTE) is often the first-line
modality for detecting cardiac hydatid cysts. It allows real-time
assessment of cyst location, internal structure, wall calcification, and
relation to adjacent cardiac chambers. On echocardiography, cardiac
hydatid cysts typically appear as anechoic or hypoechoic, welldefined,
multiloculated cystic masses, occasionally with internal
septations or “daughter cysts” [6]. Calcification may be seen as
echogenic foci along the cyst wall. In our patient, TTE revealed a wellcircumscribed
multiloculated cyst in the left ventricular wall with
peripheral calcifications and another similar lesion in the pericardial
space without hemodynamic compromise.In their review, [3] emphasized echocardiography as a critical
diagnostic tool in early detection, particularly for intramyocardial
cysts. However, visualization may be limited in posterior or apical
regions, prompting the use of additional cross-sectional imaging.
CT Findings:
Cardiac CT, particularly contrast-enhanced cardiac CT,
is pivotal in assessing the anatomical detail and complications
of cardiac hydatidosis. The typical CT appearance is that of a
well-defined, hypodense, non-enhancing cystic lesion with a
multiloculated configuration and calcified margins. CT is superior
to echocardiography in detecting wall calcifications and pericardial
involvement. It is also valuable in preoperative planning, especially
when vascular or coronary artery encroachment is suspected [6].In our case, non-contrast and contrast-enhanced CT revealed
two well-marginated, non-enhancing multiloculated cystic lesions,
one in the mid-lateral wall of the left ventricle showing peripheral
calcifications and the other in the left lateral pericardial space,these
findings are consistent with the typical CT morphology described
by Dursun et al. (2008) [6], who reported that calcified cyst walls
and internal septations are hallmark signs of hydatid disease on CT.
The lack of enhancement helped differentiate the lesions from solid
cardiac neoplasms.
MRI Findings:
Cardiac MRI is regarded as the most sensitive modality for
characterizing hydatid cysts due to its superior soft tissue contrast,
multiplanar capabilities, and ability to differentiate cystic from
solid lesions. On T1-weighted sequences, hydatid cysts are typically
hypointense, while on T2-weighted images, they appear markedly
hyperintense, reflecting their fluid content. The presence of a
hypointense rim (“pericyst”) may be seen. Internal septations and
daughter cysts further support the diagnosis [6,7].Our patient’s MRI findings corroborated these classic imaging
features: both lesions appeared hyperintense on T2-weighted
sequences without any solid components, suggesting a purely cystic
nature. The absence of pericardial thickening or effusion further
excluded constrictive pericarditis.
In a systematic review by Banisefid et al. (2023) [7], MRI was
highlighted for its ability to detect small cysts, distinguish hydatid
cysts from thrombi or neoplasms, and assess involvement of
surrounding myocardium and pericardium. Additionally, the MRI
“snake sign” or “floating membranes” can be seen in complicated or
ruptured cysts, although not present in our case.
Differential Diagnosis and Diagnostic Integration:
The differential diagnosis for intracardiac cystic lesions includes
congenital cysts, thrombi, neoplasms (e.g., myxomas, cystic tumours),
and infectious granulomas (e.g., tuberculomas).Differentiation from other intracardiac cystic lesions was essential. The non-enhancing nature on contrast CT and MRI ruled out vascularized neoplasms such as myxomas or cystic tumours. Absence of solid components and lack of gadolinium enhancement further excluded malignant masses. Thrombi were considered unlikely due to the well-defined, multiloculated morphology and peripheral calcifications, atypical for thrombotic material. Congenital cysts (e.g., pericardial cysts) were ruled out based on the bilateral (intramyocardial + pericardial) distribution, which is highly atypical. These features collectively pointed toward hydatid disease.
While serological tests (ELISA, indirect hemagglutination)
support diagnosis, they may have limited sensitivity in isolated
cardiac disease [1,2]. Hence, imaging remains the cornerstone for
diagnosis, monitoring, and pre-surgical planning.
Conclusion
Intracardiac hydatid cysts are rare but can lead to significant
morbidity if undiagnosed or untreated. Multimodal imaging plays
a pivotal role in accurately identifying cardiac and pericardial
involvement, guiding diagnosis, and aiding in preoperative planning.
Through detailed imaging findings and clinical correlation, this
case highlights the importance of considering hydatid disease in the
differential diagnosis of intracardiac masses, especially in endemic
regions or in patients with occupational exposure.
Early diagnosis and appropriate surgical intervention can
significantly reduce morbidity and improve outcomes in such rare
cases.
Acknowledgments
We would like to thank the patient for his cooperation
and providing consent to share the details of this case. We also
acknowledge the support of our colleagues and technicians in the
Department of Radiology and Cardiology for their valuable input and
assistance in the diagnosis and management of this case.
Conflicts of Interest:
We declare that there are no conflicts of interest related to this
case report.References
Citation
Bharti AS, Kumar A, Shreya, Jahan A. Rare Coexistence of Left Ventricular and Pericardial Hydatid Cysts: A Multimodal Imaging Case. Indian J Appl Radiol. 2025;11(1): 212.