Case Report
Mandibular LCH Masquerading as Parotid Enlargement: A Diagnostic Challenge
Pathapati D1*, Chandh JS2, Chandrasekhran A3 and Sistla A4
1Department of Radiology, KIMS hospital enterprises pvt.ltd, Kondapur, Hyderabad, Telangana, India
2Department of Radiology, KIMS hospital enterprises pvt.ltd, Kondapur, Hyderabad, Telangana, India
3Department of Neonatology, KIMS hospital enterprises pvt.ltd, Kondapur, Hyderabad, Telangana, India
4Department of Pathology, Apollo hospitals, Jubilee hills, Hyderabad, Telangana, India
2Department of Radiology, KIMS hospital enterprises pvt.ltd, Kondapur, Hyderabad, Telangana, India
3Department of Neonatology, KIMS hospital enterprises pvt.ltd, Kondapur, Hyderabad, Telangana, India
4Department of Pathology, Apollo hospitals, Jubilee hills, Hyderabad, Telangana, India
*Corresponding author:Deepthi Pathapati, Department of Radiology, KIMS hospital enterprises pvt.ltd, Kondapur,
Hyderabad, Telangana, India. E-Mail Id:deepthipathapati82@gmail.com
Copyright: © 2025 Pathapati D, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is
properly cited.
Article Information:Submission: 19/12/2024; Accepted: 15/01/2025; Published: 20/01/2025
Abstract
Langerhans Cell Histiocytosis (LCH) is an uncommon disorder marked by the proliferation of specialized dendritic cells that can
infiltrate various organs. Characterized by its diverse clinical presentations, LCH most frequently appears as solitary eosinophilic
granulomas in bone, primarily affecting children. Despite its rarity, with an incidence ranging from 2 to 5 cases per million annually, LCH can present at any age and often mimics other conditions, making accurate diagnosis challenging. Clinical manifestations may vary widely, from localized bone lesions to systemic involvement.
In pediatric patients, LCH can present as unifocal bone lesions, often leading to misdiagnosis if not thoroughly evaluated. A case in point is an 18-month-old female who presented with a progressive swelling in the left cheek, initially suspected to be a dental infection.
Subsequent imaging and biopsy confirmed the diagnosis of unifocal LCH of the mandible. This case highlights the importance of considering LCH in differential diagnosis, especially when dealing with atypical bone lesions in children
In pediatric patients, LCH can present as unifocal bone lesions, often leading to misdiagnosis if not thoroughly evaluated. A case in point is an 18-month-old female who presented with a progressive swelling in the left cheek, initially suspected to be a dental infection.
Subsequent imaging and biopsy confirmed the diagnosis of unifocal LCH of the mandible. This case highlights the importance of considering LCH in differential diagnosis, especially when dealing with atypical bone lesions in children
Keywords:Langerhans Cell Histiocytosis; Eosinophilic Granuloma; Mandibular Lesion; Pediatric Bone Disease; Ameloblastoma.
Introduction
Langerhans cell histiocytosis (LCH) is a rare systemic disorder
characterized by idiopathic proliferation of histiocytes, called
Langerhans cells, in different organs including the bones, lungs,
central nervous system, liver and spleen, skin, thymus and lymph
nodes. The severity and clinical behaviour depend on the number
and type of organ systems involved. Skeletal involvement is common
and may affect one or multiple bones. Involvement of a solitary bone
was previously referred to as eosinophilic granuloma (EG) and is
the most common presentation of LCH in children.[1]LCH is not
common disease with reported incidence of 0.2 – 2.0 cases per one
lakh children under fifteen years old.[2] Clinical presentations of
LCH can range from localized bone lesions to severe multisystem
involvement, which can be potentially life-threatening. Diagnosing
LCH requires a thorough approach that includes clinical examination,
histopathological studies, immunohistochemical tests, and imaging
techniques. Plain radiography, computed tomography and magnetic
resonance imaging are the most used techniques for detection and
characterization of the lesion. While the outlook is generally positive,
especially for children, there remains a significant risk of relapse and
complications, particularly in cases with multisystem involvement.
This article details the case of an 18-month-old female child diagnosed
with unifocal bony Langerhans Cell Histiocytosis (LCH), specifically
affecting the mandible.
Case Presentation
We present a case of Eighteen months old girl who was brought
to our hospital with a rapidly growing swelling on her left cheek that
had been present for more than three weeks. She had a fever one week
earlier but had not experienced any weight loss or reduced appetite.
On physical examination, a hard non-tender swelling was noted
on her left cheek. Suspecting a potential parotid gland pathology,
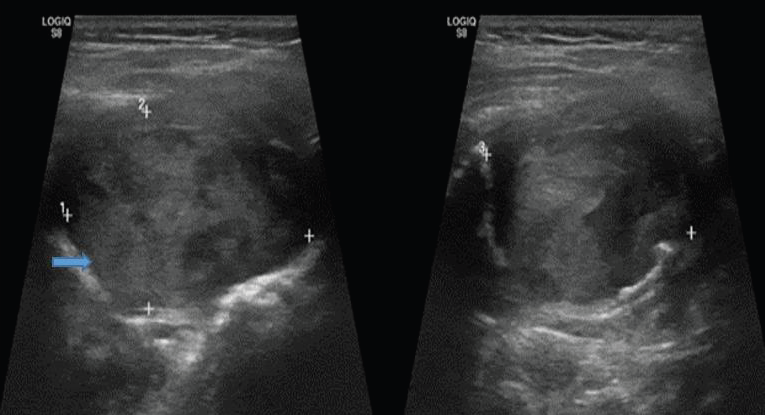
the clinician recommended an ultrasound of the neck.Ultrasound
revealed a well-circumscribed, expansile mass in the body of left
mandible with low echogenicity and internal vascularity. The lesion
caused significant destruction of both the cortical and medullary
bone surfaces of the mandible [Figure 1a] and [Figure 1b]. Suspecting
mandibular pathology, further imaging was advised. The CT imaging
revealed a large, well-defined expansile lytic lesion involving the ramus
and mandibular condyle on the left side, with extension to the TM
joint and associated cortical discontinuity[Figure 2a,b] and
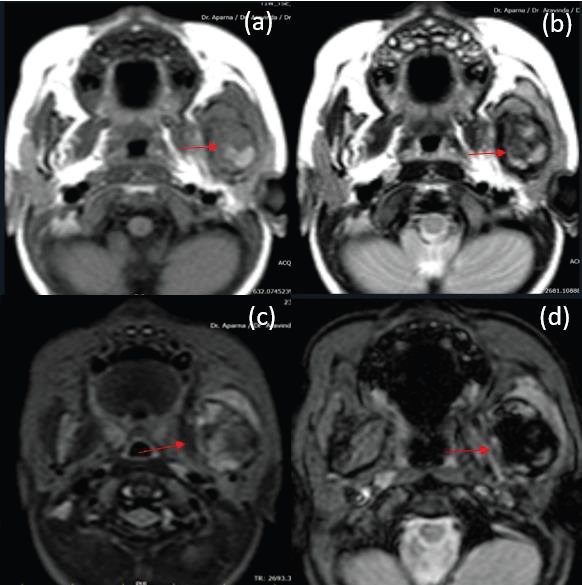
[Figure 2c]. To know the soft tissue extension, MRI neck with contrast
was done which revealed ill-defined, expansile altered signal intensity
lesion in the left mandible, extending from the angle of the mandible
to the condylar and coronoid processes. The lesion is associated
with significant cortical thinning and was in close proximity to the
masseter muscle, with a discernible loss of the fat plane separating the
lesion from the adjacent muscle.Post-contrast imaging shows subtle
enhancement of the lesion. The overlying muscle of mastication shows
T2 hyperintensity with thickening and enhancement, consistent with
inflammation or infiltration. The parotid gland is separately visualized
and does not appear to be involved by the lesion [Figure 3a-d].
Differential Diagnosis considered were Langerhans Cell Histiocytosis
(LCH), osteomyelitis, Ewings sarcoma and Ameloblastoma .
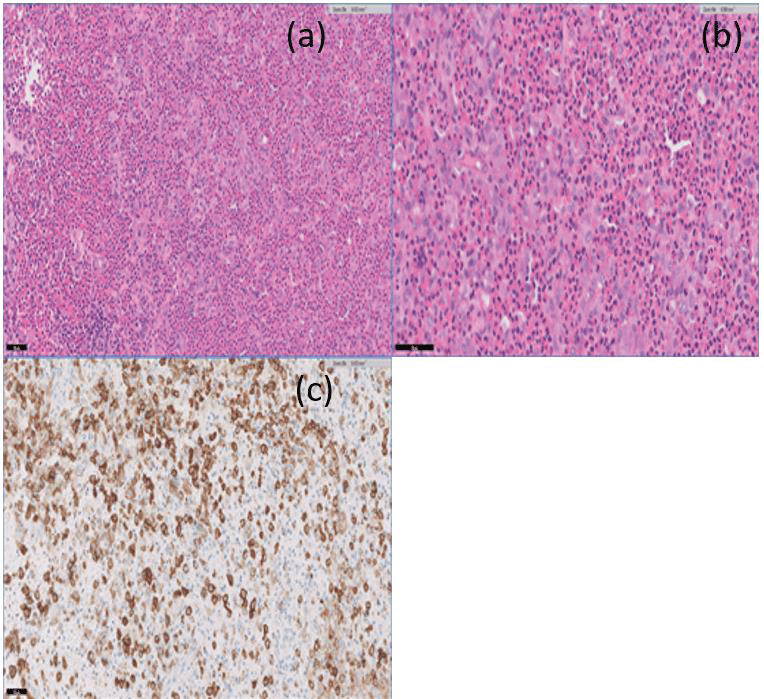
Ultrasound guided biopsy was done [Figure 4]. Samples were sent
for HPE examination. Histological features were s/o Langerhan cell
histiocytosis and subsequent IHC was positive for S100 and anti-CD-
1a [Figure 5].


Discussion
Histiocytosis is a term that refers to a group of rare disorders of
the reticuloendothelial system. LCH is associated with proliferation
of specialized bone marrow‑derived antigen presenting dendritic
cells, namely the Langerhans cells and mature eosinophils.[3] The
relative incidence of organ system involvement in LCH is as follows:
bone in 80% of the cases; skin 60% of the cases; liver, spleen, and
lymph nodes 33%; lungs and orbit in around 25% of the cases; and
maxillofacial in around 25% of the cases. Skeletal involvement can
involve any bone, but the most common are pelvis, ribs, skull, long
bones, vertebra, and facial bones. In the skull, frontal and parietal
bones are commonly involved followed by the jaws.[3] Mandible is
more commonly involved when compared to the maxilla [4]In the
present case, only the posterior aspect of the mandible was involved.
While the condition is uncommon, its presentation in the mandible
aligns with the literature indicating that the mandible is the second
most common site of osseous involvement in LCH, following the
calvarium.[1]
Based on the age, rapidly aggressive nature, clinical presentation,
and radiological features, a differential diagnosis of Ewing’s sarcoma,
LCH, and nonsuppurative osteomyelitis was considered. Both Ewing’s
sarcoma and LCH show similar radiological appearance. Ewing’s
sarcoma usually affects long bone and very rarely affects the mandible.
The other possible diagnosis is nonsuppurative osteomyelitis based on
the history of fever, nature of the lesion, and moth‑eaten appearance
of the mandibular ramus area noticed in the CT scan. Imaging plays
important role in diagnosing bone lesions, particularly CT and MRI
where we can know the characteristics, extent and adjacent soft tissue
involvement which will help in narrowing down the differentials and
in management.[5]
Histopathological analysis is critical for accurate diagnosis. LCH
presents as a diffuse infiltration of pale‑staining mononuclear cells
that resemble histiocytes with indistinct cytoplasmic borders and
rounded vesicular nuclei. Multiple eosinophils can be seen typically
interspersed among the histiocytes, plasma cells, lymphocytes, and
multinucleated giant cells.[6] In our case, similar histopathological
features were noticed with IHC positive for S‑100 and anti‑CD‑1a
[6] LCH is characterized by antigen Ki‑67 that selectively binds
to a nuclear antigen which is only expressed by proliferating cells.
[7] These characteristic features help differentiate LCH from other
conditions with similar radiological presentations.
Treatment strategies for LCH vary based on disease extent and
location. For isolated bone lesions, conservative approaches such as
surgical curettage and local steroid injections are often effective. In
contrast, multisystem disease may require more intensive treatments,
including systemic chemotherapy, radiotherapy, and/or surgery[8,9].
Conclusion
Unifocal LCH of mandible in an infant is a rare condition with a
reported incidence of 0.2 - 2.0 cases per 1,00,000 children under 15
years old, but an important diagnosis to consider when evaluating
mandibular lesions in children. The clinical presentation, radiological
features, and histopathological findings are crucial for distinguishing
it from other pathologies. Early diagnosis and prompt treatment are
essential to prevent complications such as extensive bone damage
and facial disfigurement. Regular follow-up and a comprehensive
treatment approach are necessary to manage the condition effectively
and ensure favourable outcomes.
References
Citation
Pathapati D,Chandh JS, Chandrasekhran A, Sistla A. Mandibular LCH Masquerading as Parotid Enlargement: A Diagnostic Challenge. Indian J Appl Radiol. 2025;11(1): 207.