Case Report
Cervical Rib: A Hidden Culprit in Arterial Thoracic Outlet Compression Syndrome
Poornima GB, Madhu Shankar K, Sindhu K, Naveen D, Vishwapremraj, and Mallikarjunappa B
Department of Radiodiagnosis, Sapthagiri Institute of Medical Sciences and Research Centre, Bangalore, Karnataka, India
*Corresponding author:Naveen D, Department of Radiodiagnosis, Sapthagiri Institute of Medical Sciences and Research Centre, Bangalore, Karnataka, India, Email Id: drnaveen4@yahoo.com
Copyright:© 2024 Poornima GB, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information:Submission: 11/03/2024; Accepted: 02/04/2024; Published: 08/04/2024
Abstract
Thoracic outlet syndrome (TOS) is a rare condition caused by compression of the neurovascular structures as they pass through the thoracic outlet. One uncommon but potentially serious cause of TOS is compression of the subclavian artery by a cervical rib. We present a case of a 65year-old female patient
who presented with symptoms of arm pain, burning sensation, and discolouration of right hand. Imaging studies revealed a cervical rib causing significant compression of the proximal subclavian artery, leading to arterial type of thoracic outlet syndrome. The patient underwent emergency brachial embolectomy with successful resolution of symptoms. This case highlights the importance of considering cervical rib compression in the differential diagnosis of TOS and the effectiveness of surgical intervention in such cases.
Keywords:Thoracic Outlet Syndrome; Subclavian Artery Compression; Cervical Rib; Brachial Embolectomy
Introduction
A group of disorders associated with thoracic outlet syndrome
(TOS) are brought on by compression of the neurovascular structures
that passes via the thoracic outlet. Thoracic outlet serves as the
passage that contains the brachial plexus, subclavian artery, and
subclavian vein. The compression of any of these structures by any
means can cause symptoms in the upper-extremity [1].Compression
of the neurovascular bundle at the thoracic outlet is hypothesized
to be the cause of a cluster of symptoms that includes paraesthesia,
weakness, and arm pain [2]. Atheromas can develop from persistent
compression of the subclavian artery, harming the intima and
potentially triggering anterograde or retrograde thromboembolic
episodes [1].
This report describes a case of arterial type TOS that resulted
in anterograde thromboembolic episode-induced thrombus in the
brachial artery.
Case Report
A 65-year-old female patient was referred to the surgical
department from another hospital with complaints of right upper
limb pain for two months that had gotten worse in the last week. She
has also complained of a burning sensation in her right hand with
discolouration for the past three days. She underwent an outside
Doppler scan of her right limb, which showed full occlusion of the
brachial artery distal to the mid arm and extending to the cubital
fossa, with no flow seen in the radial and ulnar arteries. The patient
appeared to be normal two months ago until he had pain in his right
upper limb, which is insidious in onset and gradually progressing.
There was no aggravating or relieving factor, and no substantial
medical, surgical, or familial history. On clinical examination, the
right upper limb was cold from the upper arm to the forearm, with no
palpable radial artery pulse and no sensation or capillary filling in the
fingertips. The patient was clinically diagnosed with peripheral arterial
disease of the right upper limb and advised to get a chest radiograph
and a CT angiogram of the right upper limb arteries in order to assess
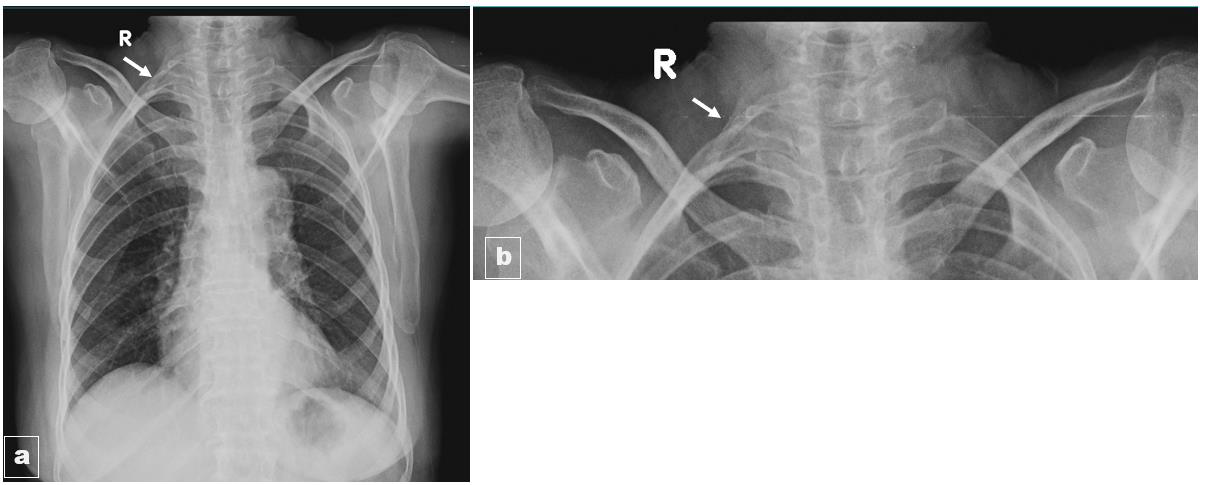
the extent of occlusion. On a routine chest radiograph, there was a
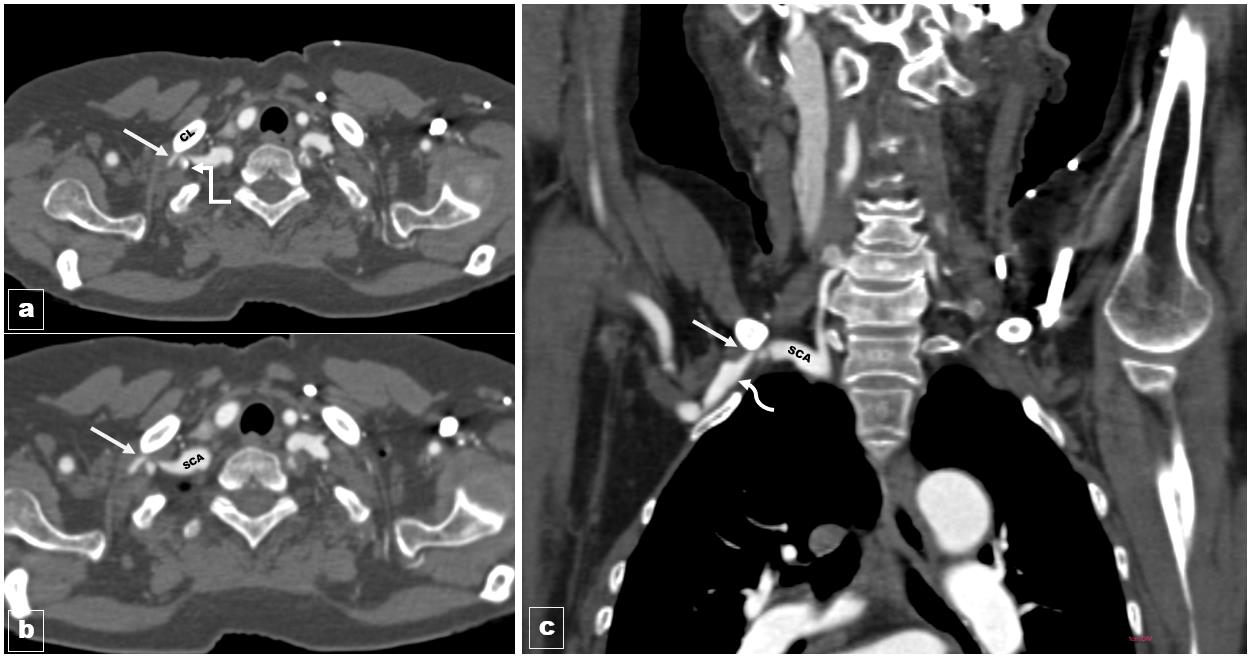
right-sided cervical rib [Figure 1]. A CT angiography revealed a rightsided
cervical rib causing compression of the proximal subclavian
artery
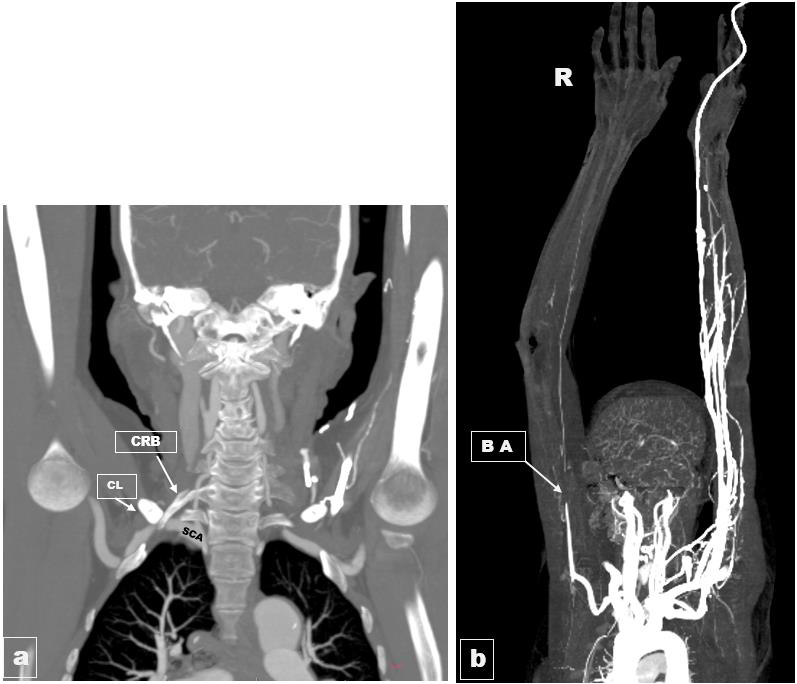
[Figure 2,3]. The proximal portion of the right
subclavian artery is substantially compressed (>90% luminal stenosis)
between the tip of the cervical rib and the clavicle, with extensive
post-stenotic dilatation of the subclavian artery. Complete luminal
occlusion of the brachial artery from the midarm to the elbow area
was caused by thrombus, and the ulnar and radial arteries showed
a marked decrease in calibre with non-opacification. With these
imaging results, the final diagnosis of subclavian artery compression
thoracic outlet syndrome caused by cervical rib was made. Later, the
patient underwent an emergency right brachial embolectomy and
recovered well after the embolectomy. The patient was recommended
to undergo resection of the cervical rib and first rib, but she chose not
to proceed with the surgery. Subsequently, we lost contact with the
patient and were unable to continue her follow-up.
Discussion
Thoracic outlet syndrome (TOS) is categorized into three
primary types: neurogenic, venous, and arterial. Neurogenic TOS
is by far the most common, that is, accounting for around 95% of
documented cases, whereas vascular causes are far less common, with
4% attributed to venous and 1% arising from an arterial etiology [2].
The costoclavicular space is the most common location for vascular
compressions, while the retropectoralis minor space is rarely a site of
compression.In cases where vascularinvolvement is suspected, further
investigation is necessary since treating the vascular compression
and related problems early on is crucial to averting infrequent but
disastrous clinical outcomes. These include pulmonary embolism and
venous gangrene of the hand due to venous TOS or digital ischemia,
as well as stroke caused by emboli from the injured Subclavian
artery [3]. Arterial TOS comprises of two components: damage to
the subclavian artery at the first rib level and distant embolic events.
Arterial TOS is nearly invariably accompanied with underlying bone
anomalies, either a cervical rib, anomalous first rib, or the first rib or
clavicle fracture [4].
Thoracic outlet syndrome is most commonly caused by cervical
ribs, especially the arterial type, which affects 85% of patients. Patients
with arterial TOS have no symptoms until a thromboembolic event
occurs. Anterograde or retrograde thromboembolism can result from
post-stenotic dilatation-induced thrombus and pseudoaneurysm
formation. Patients with thoracic outlet syndrome of the arterial
type frequently exhibit signs of artery stenosis and limb ischemia,
including pain, weakness, and cold limb [1]. Arterial TOS can present
clinically as palpable supraclavicular pulse, abnormal skin colour
changes, absent or diminished pulses, and digit ischemia. Retrograde
embolism can potentially lead to cerebrovascular accident, albeit this
is not common [1].
A thorough history, physical examination (including provocative
tests), radiography, electrodiagnostic testing, and brachial plexus
neurography are often used in the diagnosis of TOS. Nonetheless,
imaging modalities may help in the diagnosis of patients if there is
a suspected vascular component [3]. CT scans and MRIs are often
regarded as the best diagnostic tools for thoracic outlet syndrome.
Finding the pathological or anatomical root cause of TOS is the aim of
imaging techniques. Vascular TOS is diagnosed when the subclavian
artery or vein narrows by more than 30% or 50%, respectively.
Imaging findings associated with arterial TOS include localized fixed
stenosis of the subclavian artery on the compression side, arterial
thrombosis, and the development of aneurysms or pseudoaneurysms
in the axillo-subclavian artery [1,4,5].
The management of a TOS is not uniform and is mostly
determined on the underlying cause. Conservative management or
surgery, such as surgical bypass, rib resection, scalene resection, as
well as endovascular repair, are available options[2,6].
Conclusion
Arterial thoracic outlet syndrome (TOS) is often associated with
bone anomalies like a cervical rib, an anomalous first rib, or fractures
of the first rib or clavicle. When vascular involvement is suspected,
radiological examinations play a crucial role in identifying the cause
of arterial TOS and planning appropriate treatment to relieve vascular
compression and its potential complications, thereby preventing rare
but serious clinical outcomes.
Consent: The patient has given her consent for hercross-sectional
images and other clinical information to be reported in the journal.
The patient is aware that her name and initials won’t be revealed in
the publication.