Case Report
Novel Case of X-configured Stenting in India for the Treatment of Wide-Necked Anterior Communicating Artery Aneurysm along with Anterior Communicating Artery Complex Reconstruction
Ritu S and Rashmi S*
Seth GS Medical College and King Edward Memorial Hospital, Maharashtra, India
*Corresponding author:Rashmi S, Seth GS Medical College and King Edward Memorial Hospital, Maharashtra, India, E-mail Id: drrashmisaraf@gmail.com
Copyright:© 2024 Ritu S, et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information: Submission: 15/12/2023; Accepted: 29/01/2024; Published: 05/02/2024
Abstract
A 39-year-old male presented with a severe holocranial headache and vomiting since 1 day. CT showed diffuse SAH, DSA depicted an extremely wide-necked anterior communicating artery aneurysm incorporating bilateral A2 segment origins. The aneurysm measured 8x6x7mm, with a neck measuring 7mm. It was directed infer medially with a part of fundus superior to the anterior communicating artery
region.
Attempt to cannulate the ipsilateral A2 segments from each of the A1 segments was unsuccessful. Due to wide-neck, acute A1-A2 angle and bilateral incorporation of the A2 segments, treatment plan was changed to X-stenting. Wire was cannulated from right A1 to left A2, and second microcatheter was placed from left A1 to right A2. Another microcatheter was negotiated from the left ACA into the aneurysmal sac. 2 stents measuring 3x18mm and 3x24mm were deployed in an ‘X’-fashion. Subsequently, aneurysm was coiled through jailed microcatheter with 3 detachable platinum coils.
Post-procedural angiography showed minimal residual opacification of inferior sac with patent stented segment and distal ACAs.
There was good reconstruction of the anterior communicating artery complex.
Repeat angiography on day 7 showed exclusion of the inferior sac of the aneurysm with minimal neck residual opacification.
Follow-up CT angiography done at three months showed good patency of stents. Control DSA at 6 months showed complete exclusion of aneurysm with patent stents. At two years, patient was clinically stable and asymptomatic.
This case illustrates the advantage of X-stenting for embolization of large, wide-neck, bilobed aneurysms with acute A1-A2 angle as an alternative to traditional treatment modalities.
To the best of our knowledge, this is the first reported case of ‘X-stenting’ for anterior communicating artery aneurysm in India.
Keywords:X-Stenting; Cross-Stenting; Anterior Communicating Artery Aneurysms; Acomaa; Endovascular Techniques
Case Report
A 39-year-old male presented with a severe holocranial headache
and vomiting since 1 day. On observation, no focal neurological
deficits were present. Computed Tomography showed diffuse
subarachnoid haemorrhage, and Digital Subtraction Angiography
depicted an extremely wide-necked anterior communicating
artery aneurysm incorporating the origin of bilateral A2 segments.
The aneurysm measured approximately 8 x 6 x7 mm in diameter
with a neck measuring about 7mm. It was directed predominantly
inferomedially with a part of the fundus superior to the anterior
communicating artery region.
The patient was prepared for stent implantation and coil
embolization. Two hours preoperatively, the patient was put on 2
tablets of Ticagrelor 90mg and 150mg of aspirin. Under general
anaesthesia, a short 8F sheath was placed in the groin, through
which 6F Neuron Max Long sheath (80 cm) and Neuron Max 070
introducer were guided to the right common carotid artery from right
transfemoral approach; and to the left common carotid artery from
left transfemoral approach respectively. Neuron guiding catheter was
placed in both cervical internal carotid arteries. Headway 17 micro
catheter was negotiated into the A1 segments bilaterally.
An attempt to cannulate the ipsilateral A2 segments was made
from each of the A1 segments. Due to the wide neck of the aneurysm,
acute A1-A2 angle and bilateral incorporation of the A2 segments,
the treatment plan was changed to X-stenting. So instead, the wire
was cannulated from right A1 to left A2, and another microcatheter
was placed from left A1 to right A2. A third microcatheter was
negotiated from the left anterior cerebral artery into the aneurysmal
sac. 2 stents measuring 3mm x 18 (Microvention Terumo Lvis Junior)
and 3mm x 24 (Microvention Terumo Lvis Junior) were deployed in
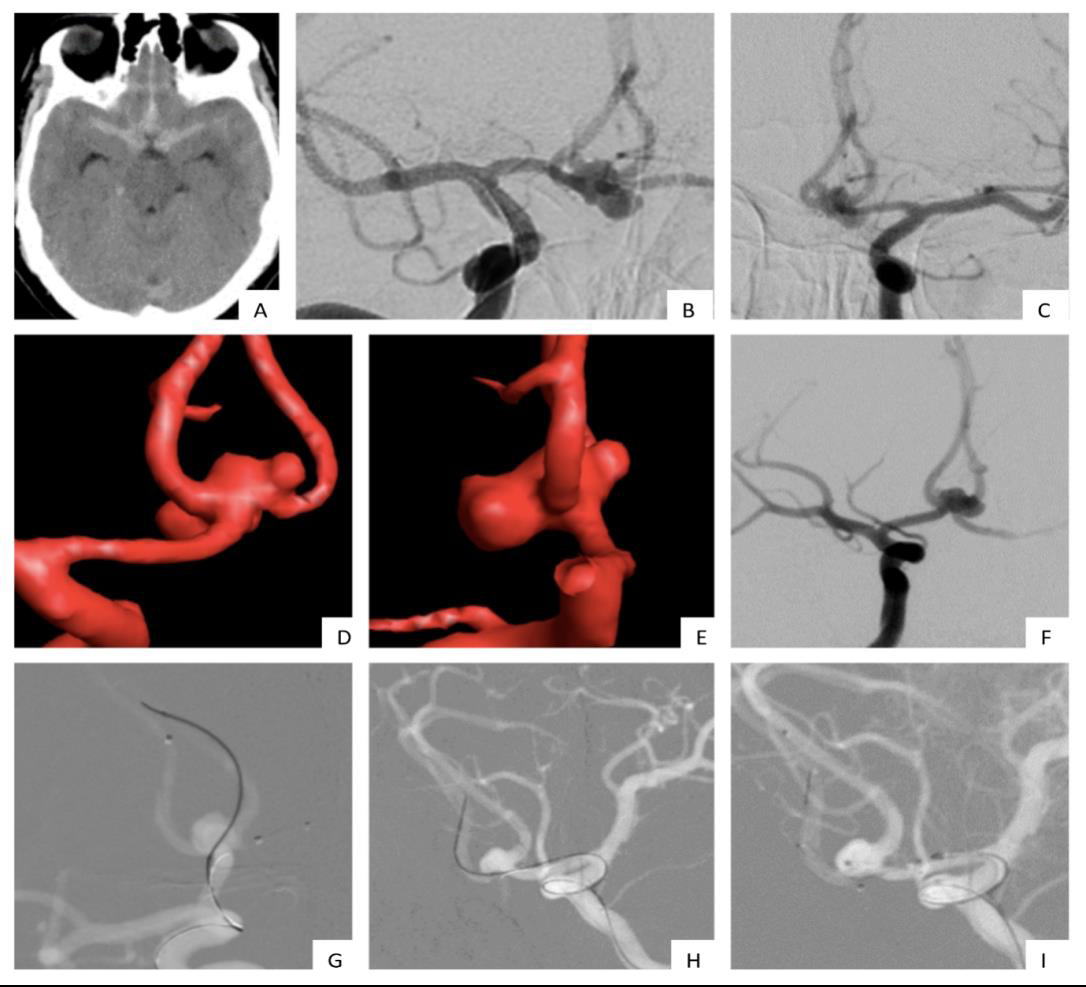
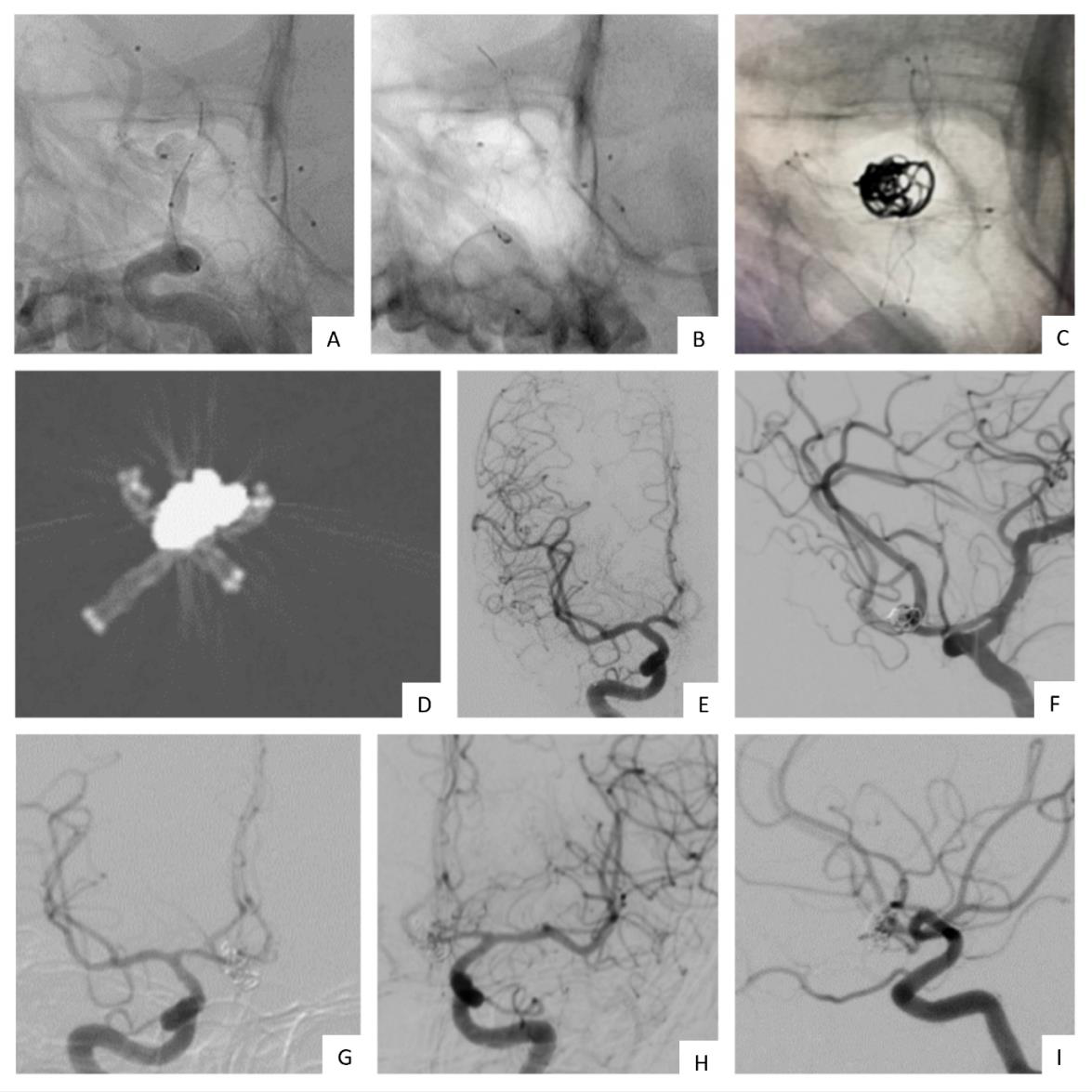
an ‘X’ fashion. Subsequently, coiling was performed through jailed
microcatheter using three detachable platinum coils (Microplex,
Microvention Terumo). Hemostasis at the puncture site was achieved
by direct compression.
Post-procedural angiography showed minimal residual
opacification of the inferior sac with good patency of the stented
segment and distal anterior cerebral arteries. There was good
reconstruction of the anterior communicating artery complex. The
patient was extubated without complications and monitored in the
ICU for a week.
Repeat angiography was done on day seven at the time of
discharge and showed exclusion of the inferior sac of the aneurysm
with minimal neck residual opacification.
Follow-up CT angiography was done at three months and showed
good patency of stents. Control DSA at six months showed complete
exclusion of aneurysm with patent stents. At two years, the patient
was clinically stable and asymptomatic.
Discussion
Anterior communicating artery aneurysms are the most
commonly occurring intracranial aneurysms, accounting for 23-40%
of all ruptured aneurysms and 12-15% of unruptured aneurysms [1].
Due to their complex arterial relationships with perforators and
higher potential of cognitive dysfunction with microsurgical clipping,
endovascular therapy has become the treatment of choice for these
aneurysms [2].Wide aneurysmal neck has been identified as a limiting
factor for endovascular coiling. This difficulty has been tackled by
using remodeling neck techniques (using balloons), simultaneously
deploying 2 coils at the beginning of framing of the aneurysm, or by
use of multiple stents [3]– as seen in our case.
A small increase in aneurysmal diameter leads to a fourfold
increase in neck surface area. Because of the significantly larger neck
surface area in wide necked aneurysms – coils seek the path of least
resistance and herniate into the parent vessel if simple endovascular
coiling is attempted – hence, methods such as X-stenting must be
employed in these cases. Wide-necked aneurysms are more likely to
require retreatment because of coil compaction on follow-up – this
is due to the inability to protect the parent vessel and, therefore, the
inability to densely pack the aneurysm [4].
Moon et al. reviewed the long-term prognosis of patients enrolled
in the Barrow Rupture Trial(BRAT) and found that 16.9% of the 39
patients included in the endovascular group had to be transferred to
the surgical clipping group due to embolization difficulties [5].
The small length of the AcomA along with the acute angle of
adjacent vessels make it very difficult to use balloon- or stent-assisted
techniques. This limitation is because the inability to reach parent
vessel at aneurysmal neck and loops in internal carotid arteries may
prohibit stent or balloon navigation. Additionally, if the aneurysm is
extremely wide-necked as in our case, a balloon would not be enough
to prevent coil protrusion in the parent artery [2].
In a study comparing stent-assisted coiling and balloon-assisted
coiling for wide neck aneurysms conducted in 101 consecutive
patients, Chalouhi et al. found that the use of stents was associated
with lower rates of retreatment, and higher rates of aneurysm
obliteration and progression of occlusion at follow-up[6].
Self-expanding stents can be used for complex, wide necked
aneurysms to achieve more durable long-term results.They are
preferred for not only the scaffold they provide, but they also achieve
better initial occlusion rates while sparing parent artery lumen and
to decrease likelihood of re-growth – this is due to the alteration they
create in intraaneurysmal hemodynamics [7].
Saatci et al. conducted X-stenting in 5 wide necked
AcomAAincolving both A1-A2 junctions, with 100% technical
success and no re-growth on follow up at 6 months.
In our study, the attempt to cannulate ipsilateral A2 from A1
was made but was unsuccessful due to the wide neck, sharp A1-A2
angle and bilateral incorporation of A2 segments. Hence, this plan
of “opposite L configurations” was abandoned and X-stenting was
preferred. Alteration of flow direction at the aneurysmal neck, which
is found to have an impact on long term re-growth rates, is more
efficient with X-stenting rather than “opposite L” configurations[7].
Another advantage of X-stenting is that the patency of the
reconstructed AcomA is preserved. Conversely, it is only an option
for patients with good sized A1s on either side. If there is hypoplastic
A1 on one side, Y-stent placement through the large-sized A1 is the
treatment of choice[7].
In acute/subacute phase of rupture – there is moderate to severe
vasospasm, hence the stent should be oversized. Open-cell design
stents show increased opening of cells and outward prolapse of
struts into aneurysmal neck, thereby reducing largest diameter of
aneurysmal sac – hence, coils should be undersized [2].
We used the ‘jailing of micro catheter’ technique – which permits
stabilization of the coil during delivery. This technique is unsuitable
for cases with small diameter of ACA [2].
In our patient, X-configured stent assisted coiling was used
successfully for a very wide neck aneurysm with bilateral incorporation
of A2 segments. This techniqye creates a different flow status change,
which is postulated to decreased re-growth or recurrence of the
aneurysm.
Control DSA at six months showed complete exclusion of
aneurysm with patent stents. At two years, the patient was clinically
stable and asymptomatic.
X-configured stent-assisted coiling is technically feasible in the
treatment of wide necked AcomAA with acute A1-A2 angle and
bilateral incorporation of A2 segments.
To the best of our knowledge, this is the first reported case of
‘X-stenting’ for anterior communicating artery aneurysm in India.
Ethical Considerations:
A. Ethical approval: All procedures performed in studies
involving human participants were in accordance with the
ethical standards of the institutional and/or national research
committee and with the 1964 Helsinki declaration and its
later amendments or comparable ethical standards.
B. Informed consent: Informed consent was obtained from the
individual included in the study.
C. Conflict of interest: The authors have nothing to discloseReferences
Citation
Ritu S, Rashmi S. Novel Case of X-configured Stenting in India for the Treatment of Wide-Necked Anterior Communicating Artery Aneurysm along with Anterior Communicating Artery Complex Reconstruction. Indian J Appl Radiol. 2024;10(1): 190.