Case Report
Imaging in Disseminated Cysticercosis: A Case Report and Review of Literature
Tejas Mohan Tamhane*, Sushil Ghanshyam Kachewar, Dilip L Lakhkar
Corresponding author: Tejas Mohan Tamhane, Department of Radio-Diagnosis, PDVVPF’S Medical College andHospital, Vilad Ghat, Ahmednagar, Contact no. - 8275883113/ 7083770202, India; E-mail: drtejastamhane88@gmail.com
Citation: Tamhane TM, Kachewar SG, Lakhkar DL. Imaging in Disseminated Cysticercosis: A Case Report and Review of Literature. Indian J ApplRadiol. 2015;1(1): 105.
Copyright © 2015 Tejas Mohan Tamhane SG. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Applied Radiology | Volume: 1, Issue: 1
Submission: 14/09/2015; Accepted: 29/10/2015; Published: 03/11/2015
Abstract
Cysticercosis is caused by the larval form of the pork tapeworm Taenia solium. It is endemic in most parts of Asia and is transmitted by the feco-oral route. It is the most common parasitic infestation of the central nervous system.
Disseminated Cysticercosis (DCC) is an uncommon manifestation of this common disease. One such rare case, diagnosed in a child patient is reported here with a diffuse involvement of the Brain, muscles of extremities, subcutaneous tissues and intrabdominal organs.
The correct diagnosis of this case was made on the basis of high-resolution Ultrasonography of the involved parts along with a CT scan of Brain. Multiple oval cystic lesions with central scolex were noted in muscles, subcutaneous tissues and within the liver on ultrasound whereas multiple ring-enhancing lesions with perifocal edema were noted on CT Brain because of the diffuse involvement of the brain parenchyma.
Keywords: Disseminated cysticercosis; Muscle pseudohypertrophy; Neurocysticercosis; Subcutaneous nodules
Introduction
Cysticercosis is caused by cysticercus cellulosae, which is the larva of Taenia solium, the pork tapeworm. The larvae are carried inthe blood stream after penetrating the walls of the alimentary tractand they lodge in different tissues like the skin, skeletal muscles,brain, fundus and heart to cause Disseminated cysticercosis. Thoughcysticercosis is the most common helminthic infection of the CNS,disseminated cysticercosis is rare. Less than 50 cases of disseminatedcysticercosis have been reported world-wide [1].
We report here one such rare case of Disseminated Cysticercosisin a child who had recurrent seizures, headache, painful subcutaneousnodules, and muscular hypertrophy. The diagnosis in this case wasprimarily done with the help of High resolution Ultrasonographywhereas CT Brain helped in detecting the CNS involvement.
Case Report
5yr old male child resident of Bihar, recently shifted toMaharashtra, came to the Pediatric OPD with complaints of arecurrent seizures, headache, painful swellings in both the buttocks,thighs and calf region. He also complained of abdominal pain in righthypochondriac region non radiating with no aggravating or relievingfactors. There was no history of vomiting, bowel/bladder complaints.He was a non-pork eater.
Examination revealed multiple subcutaneous nodules of size 1-2cm over the lower extremities with mild hepatomegaly.
Blood Investigations showed,
Hemoglobin- 8.4mg/dl,
Total Leukocyte Count- 21000/cumm,
Platelets- 8.56lacs/cumm
Sr. Urea- 38
Sr. Creatinine- 0.6
Sodium- 133, Potassium- 4.0
Sr. bilirubin (T)-0.6 SGOT- 23
Sr. bilirubin (D)-0.2 SGPT- 19
AlKPO4- 267
Absolute Eosinophil count: 2714
He was sent to the department of Radio-Diagnosis for evaluationof muscular hypertrophy and painful subcutaneous swellings overbuttocks, thighs and calf region.
High resolution Ultrasonography of the involved muscles and abdomen was done which showed multiple oval to circular, predominantly anechoic lesions, which were around 1-2 cm in diameter. Most of these cystic lesions showed a hyperechoic focus within which is suggestive of a scolex. There was no increased vascularity surrounding the lesions on color Doppler examination.
X-Ray of extremities and chest was within normal limits. For seizures and headache, CT Brain was advised which showed characteristic cysticerci scattered in the brain parenchyma with multiple ring-enhancing lesions and perifocal edema, confirming the diagnosis of Neurocysticercosis. Thus diagnosis of Disseminated Cysticercosis was made as multiple organ systems were involved in this case.
Discussion and Review of Literature
Cysticercosis is caused by the larval form of the pork tapeworm Taenia solium. It is endemic in most parts of Asia and is transmitted by the feco-oral route.
When cysticerci involve the nervous system it is known as Neurocysticercosis (NCC). It is the most common parasitic infestation of the central nervous system.
Neurocysticercosis can present with a wide range of manifestationslike convulsions and signs and symptoms of a space-occupyinglesion. Blurring of vision can be due to a space occupying lesion(SOL) or papilledema caused by the cyst. If pericystic inflammationis absent, the NCC may be asymptomatic. Our patient had symptomsof CNS involvement like headache, Seizures which prompted us toinvestigate him for Neurocysticercosis which was confirmed with thehelp of CT Brain.
The term ‘Disseminated Cysticercosis’ was coined by Priest in1926 to refer to the presence of a multiple cysticerci in the multiplelocations like subcutaneous tissue, muscles, eyes, brain, heart etc [2].The syndrome of disseminated muscular cysticercosis is characterizedby pseudomuscular hypertrophy (100%), palpable subcutaneousnodules (87%), seizures, and abnormal mentation (78%).
Ocular involvement can be a part of the disseminated cysticercosis syndrome. Though, Ultrasound of Eye ruled out the ocularinvolvement in this patient, severe pain, blurring of vision and loss of vision are the common manifestations in such cases. Fundoscopicexamination, ultrasonography of the eyes and Color Doppler studiesare useful in diagnosing ocular cysticercosis Figure 1-3.
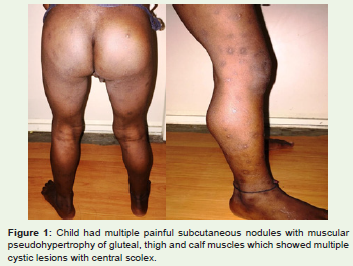
Figure 1: Child had multiple painful subcutaneous nodules with muscular pseudohypertrophy of gluteal, thigh and calf muscles which showed multiple cystic lesions with central scolex.
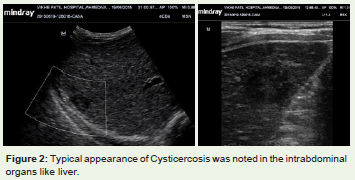
Figure 2: Typical appearance of Cysticercosis was noted in the intrabdominalorgans like liver.
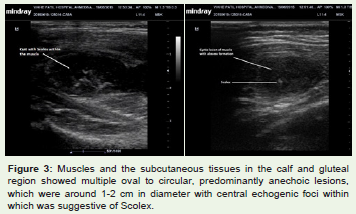
Figure 3: Muscles and the subcutaneous tissues in the calf and gluteal region showed multiple oval to circular, predominantly anechoic lesions, which were around 1-2 cm in diameter with central echogenic foci withinwhich was suggestive of Scolex.
Although, cerebral cysticercosis is common, reports ofdisseminated cysticercosis are rare. Out of 450 cases of cysticercosisreviewed by Dixon and Lipscomb [3] in 1961, only 1 case of dissemination was reported. Similarly, Kumar et al. [4] reviewed 22 cases of disseminated cysticercosis, and Satyanarayana et al. [5] reported 2 such cases.Clinically, 3 types of Cysticercosis have been described in the past by different studies:
Myalgic, myopathic type;
Nodular or mass like type;
Rare pseudohypertrophy type [6-8].
Our patient had both, the painful subcutaneous nodules and the pseudohypertrophy of the muscles of buttocks, thighs and calf.
The clinical features depend on the location of the cyst, the cyst burden, and the host reaction. Subcutaneous cysticercosis may cause painless or painful subcutaneous nodules as in our case. Muscular cysticercosis may present clinically with myalgia, pseudotumor or mass and pseudohypertrophy. Exact pathogenesis of muscular pseudohypertrophy in cysticercosis is not well known but one of the theory states that the dead larva may act as an irritant to the muscles, causing the inflammatory changes whereas response to steroids has raised the hypothesis that it may be a consequence of an allergenic response Figure 4,5.
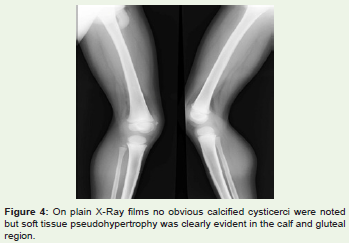
Figure 4: On plain X-Ray films no obvious calcified cysticerci were noted but soft tissue pseudohypertrophy was clearly evident in the calf and gluteal region.
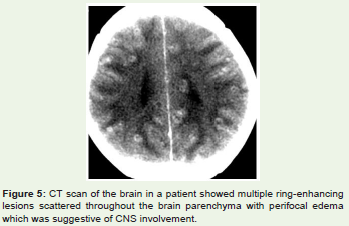
Figure 5: CT scan of the brain in a patient showed multiple ring-enhancing lesions scattered throughout the brain parenchyma with perifocal edema which was suggestive of CNS involvement.
Clinically, soft tissue cysticercosis can be misdiagnosed as lipoma, epidermoid cyst, abscess, pyomyositis, neuroma, neurofibroma, tuberculous lymphadenitis, sarcoma, myxoma, ganglion or fat necrosis [9]. Whenever patient presents with a painful or painless swelling of long duration, the clinicians should consider cysticercosis as a differential diagnosis, as it is a very common soft tissue infection. USG is the initial and one of the useful diagnostic modality for a softtissue swelling [10].
First | Type of appearance is a cysticercus cyst with an inflammatory mass around it, as a result of the death of the larva. Similar picture was observed in our case. |
Second | Appearance is an irregular cyst with very minimal fluid on one side, indicating the leakage of fluid. The eccentric echogenic protrusion from the wall due to the scolex is not seen within the cyst. This may be because the scolex escapes outside the cyst, or because of the partial collapse of the cyst. |
Third | Appearance is a large irregular collection of exudative fluid within the muscle, with the typical cysticercus cyst containing the scolex situated eccentrically within the collection. This may be due to chronic intermittent leakage of fluid from the cyst, leading to floridinflammatory exudates. |
Fourth | Appearance is of calcified cysts appearing as multiple elliptical calcifications in soft tissue similar to the pathognomonic millet seed-shaped elliptical calcifications described on plain radiograph. |
The diagnosis is relatively difficult to make solely on a clinical basis because the manifestations are not specific, and visualization of the organism usually is not feasible. Plain radiographs will show the cysticerci only when they are calcified [11]. Hence, imaging in such cases with High Resolution Ultrasonography along with CT/MRI is highly useful to come to a final diagnosis. It would be reasonable to say that high-resolution sonography can suggest the diagnosis of muscular and subcutaneous cysticercosis whenever such lesions are seen and even in cases such as disseminated cysticercosis. A case of generalized cysticercosis, can also be confirmed by muscle biopsy, as it was done in our case, which showed densely packed cysticerci in the muscles.
Different sonographic appearances of muscular cysticercosis have been described by Vijayaraghavan SB and these appearances on high-resolution sonography are pathognomonic of cysticercosis and a definitive diagnosis can be made with greater confidence [12].
Treatment of soft tissue cysticercosis depends on the locationof the cysts. Surgical excision is done for isolated skeletal muscleor soft tissue cysticercosis associated with abscess [13]. Cysts thatare not associated with abscess can be treated with antihelminthicmedications such as albendazole or praziquantel [14]. Follow-upUSG is done after three weeks of antihelminthic medication to lookfor resolution of the lesion.
Conclusion
Disseminated Cysticercosis although rare condition, needs timely diagnosis to prevent the complications. Cysticercosis, thus, should always be part of the differential diagnosis of subcutaneous and intramuscular swellings in Indian subcontinent. High Resolution USG is a good modality for diagnosing Disseminated Cysticercosis. Clinical judgment along with the various imaging modalities would ultimately help in precise diagnosis and proper treatment.
References
- Kumar A, Goenka AH, Choudhary A, Sahu JK, Gulati S (2010) Disseminated cysticercosis in a child: Whole-body MR diagnosis with the use of parallel imaging. Pediatr Radiol 40: 223-227.
- Wadia N, Desai S, Bhatt M (1988) Disseminated cysticercosis. New observations, including CT scan findings and experience with treatment by praziquantel. Brain 111: 597-614.
- Dixon HBF, Lipscomb FM (1961) Cysticercosis: an analysis and follow-up of 450 cases. Med Res Counc Rep Ser 299: 1-58.
- Kumar A, Bhagwani DK, Sharma RK, Sharma KS, Datar S, et al. (1996) Disseminated cysticercosis. Indian Pediatr 33: 337-339.
- Satyanarayana S, Gorthi SP, Bhardwaj JR, Nath N, Sharma S (2002) Disseminated Cysticercosis. J Assoc Physicians India 50: 1180-1182.
- Kazanjian PH, Mattia AR (1994) Case records of the Massachusetts General Hospital. Weekly clinicopathological exercises. Case 26-1994: a 20-year-old Philippine woman with a soft-tissue mass in the forearm. N Engl J Med 330: 1887-1893.
- Anderson GA, Chandi SM (1993) Cysticercosis of the flexor digitorum profundus muscle producing flexion deformity of the fingers. J Hand Surg Br 18: 360-362.
- Chopra JS, Nand N, Jain K, Mittal R, Abrol L (1986) Generalized muscular pseudohypertrophy in cysticercosis. Postgrad Med J 62: 299-300.
- Jhankaria BG, Chavhan GB, Krishnan P, Jhankaria B (2005) MRI and ultrasound in solitary muscular and soft tissue cysticercosis. Skeletal Radiol 34: 722-726.
- Smiti S, Sripathi H, Naik L (2003) Unusual location of cysticercus lesions in soft tissue: report of three cases. Indian J Radiol Imaging 13: 157-158.
- Schantz PM (1994) Larval cestodiasis. In: Hoeprich JD, Jordan MC, Ronald AR (eds). Infectious Diseases. 5th ed. Philadelphia, PA: JB Lippincott Co 850-860.
- Vijayaraghavan SB (2004) Sonographic appearances in cysticercosis. J Ultrasound Med 23: 423-427.
- Sidhu R, Nada R, Palta A, Mohan H, Suri S (2002) Maxillofacial Cysticercosis - Uncommon appearance of a common disease. J Ultrasound Med 21: 199-202.
- Mittal A, Das D, Aiyer N, Nagaraj J, Gupta M (2008) Masseter cysticercosis - a rare case diagnosed in ultrasound. Dentomaxillofac Radiol 37:113-116.