Research Article
Implementing One Minute Preceptor forEffective Teaching and Learning among Radiology Residents
Sushil G Kachewar*
Corresponding author: Dr. Sushil Ghanshyam Kachewar, MD, DNB, PhD, FICR, Professor, PDVVPF`s Medical College,Ahmednagar, Maharashtra, PIN- 414 111, India; E-mail: sushilkachewar@hotmail.com
Citation: Kachewar SG. Implementing One Minute Preceptor for Effective Teaching and Learning among Radiology Residents. Indian J Appl Radiol.2015;1(1): 104.
Copyright © 2015 Kachewar SG. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Applied Radiology | Volume: 1, Issue: 1
Submission: 23/07/2015; Accepted: 14/09/2015; Published: 19/09/2015
Abstract
Context: In the clinical speciality of radio-diagnosis, it is vital that the resident (post-graduate student) makes an accurate diagnosis when performing ultrasound of patients with acute abdomen. This study is aimed at teaching residents a systematic approach towards performing ultrasound in cases of acute abdomen using a new educational tool known as One Minute Preceptor (OMP) as well as assessing the usefulness of this innovative teaching-learning tool.
Methods: Residents from the Department of Radiology participated as learners and a single teacher from the same department participated as the preceptor in this study. Response from the residents was marked on the Likert Scale. The intended end point was to introduce residents to a new teaching/facilitation tool to assist them in the process of making a definite diagnosis and to test their perceptions about the influence of the new tool. To assess the effectiveness of this research, the four-level model created by Donald Kirkpatrick and Likert Scale was utilized to measure the change in attitude. The p value was calculated using the Mann-Whitney U test.
Results: The Likert item response number 1 to 4 [pre-test] had a mean value of 3.5 and item number 8 to 9 [post-test] had a mean value of > 4.5; indicating that the residents’ level of learning has significantly improved (p < 0.001). All the residents were able to satisfactorily rule in or rule out a definitive cause of pain in patients with acute abdomen with the use of ultrasound for diagnosis, compared to the pre-project status where the diagnosis was rarely definitive and was more often only speculative.
Conclusion: OMP encourages residents to think critically about the case and gives insight into clinical reasoning skills. It also reminds preceptors to provide feedback on performance.
Keywords: Medical Education Technology; Teaching-Learning Methods; One Minute Preceptor; Likert Scale; Kirkpatrick’s evaluation model
Introduction
The radiology department is one of the busiest departments in aninstitution as almost every patient is referred to this department tofind any demonstrable cause of his or her ailment. A very high numberof ultrasound referrals make it impossible for the faculty membersto scan each patient. Hence, ultrasound is most often performed byresidents undergoing post-graduate training. Traditionally, patientsare brought to the notice of the faculty only when the residentscannot reach a definitive diagnosis. The teacher then takes over the case and provides a ready-made diagnosis. Ideally, however, theteacher should have guided the resident to reach a diagnosis insteadof providing a ready-made diagnosis. The teacher takes appropriatehistory, performs relevant clinical examination and correlatesultrasound (USG) findings with those of other investigations inreaching the accurate diagnosis. Often, it is realized that, had theresidents followed this systematic approach, the diagnosis would havebeen easily made. When one or more of these steps are missed bythe residents, they cannot reach a definitive diagnosis and hence theyturn to the preceptor for guidance.
This education research project was undertaken to introduceand implement a novel method of ‘One Minute Preceptor’(OMP)in the place of traditional teaching. The ultimate aim was to makethe residents perfect in sonographically evaluating patients of acuteabdomen so that a satisfactory diagnosis could be reached. The authorhad previously conducted a study using OMP in patients presentingwith right iliac fossa pain [1].
OMP is a learner-centered model of precepting in which duringthe teaching encounter, the focus is on the learner’s reasoning whilesimultaneously gathering the necessary components of the historyand physical examination and its proper correlation with otherrelevant laboratory findings. In traditional methods of teaching, onlya small amount of the entire time is devoted for actual teaching andno constructive feedback is given [2]. OMP aims to overcome thisshortcoming. The “one-minute preceptor” is a modern teachinglearningmethodology for efficiently structuring an interaction with alearner [3]. It has been widely tested in the Western world but has notyet been introduced and implemented in this medical college.
The five steps of OMP [4-7] are as follows-
1. Get a commitment from the learner
In this first step, the resident (learner) is asked to evaluate thepatient by himself or herself without any help from the teacher(preceptor). Resident performs a thorough USG scan of the patient tothe best of his abilities. After completing the USG scan, he discloseshis observations (both positive as well as negative) and commits toa diagnosis. At times, if the resident has not reached any specificdiagnosis, the teacher asks him to commit to the most likely diagnosisor enlist the differential diagnosis.
2. Probe for underlying reasoning
Once step one is achieved and the resident commits to a diagnosis,the teacher encourages him to spell out the observations or findingswhich made the resident to commit to the diagnosis.
3. Provide positive feedback
After the resident discloses his reasoning behind the committeddiagnosis, it is now the teacher’s turn to pick up the positives from hisobservations and congratulate/appreciate him for not missing them.
4. Correct errors in reasoning
Now is the time for the teacher to disclose the errors made bythe resident. This is an art and is strictly different from criticism. Atno time in this step should the resident feel that he is being belittled.
5. Teach general rules (key teaching points)
In this last step, the teacher summarizes the entire scenario inhis language and describes how the diagnosis could be successfullyreached based on scientific reasoning. The session ends after theteacher highlights the key teaching points and makes sure thatresidents have followed them.
Methods
This scientific study aimed to investigate the utility of OneMinute Preceptor for effective teaching and learning among radiology residents. The clinical scenario of ultrasound evaluation ofa patient with acute abdomen was chosen for this study. Necessarypermission from the institutional and departmental research andethical committees was obtained. In addition, written consent wasobtained from every participant (resident).
The study extended over a duration of 3 months from May toJuly 2015. A total of 12 residents in the department of radio-diagnosisparticipated in this study as the learners while the author participatedas the sole preceptor. Each resident had at least 12 months ofexperience in performing abdominal ultrasound independently,while the teacher had an experience of 14 years.
The major tasks involved in the study were the Pre-InterventionQuestionnaire for Learner, Intervention detailing OMP, Post-Intervention Questionnaire for Learner and the subsequentstatistical analysis. The teacher in this study had undergone a basicand advanced course in medical education technology from anauthorised university of health sciences, in which he was taught OMPby the national faculty of medical education and technology unit.The teacher performed this educational exercise a total of 13 times;first as a common demonstration to all the 12 residents in the formof a PowerPoint presentation and subsequently as a demonstrationto each of the 12 residents independently. The response from theresidents was obtained on the Likert scale within 24 hours of thesession. The intended end point was to enable residents to make adefinite diagnosis after performing ultrasound in patients with acuteabdomen. OMP was the new teaching/facilitation tool to assist themin this process.
For statistical analysis the Likert scale which is a psychometricscale that captures the intensity of their feelings for a given item [8],was used [9]. Table 1 shows the proforma of questionnaire using theLikert Scale to get Learners’ response on a scale of 1 to 5; where a score of 1- strongly disagree, 2- disagree, 3-neutral, 4-agree and 5-strongly agree. The p value was calculated using the Mann-Whitney U test to assess the significance of the differences between the pre- and posttest results.
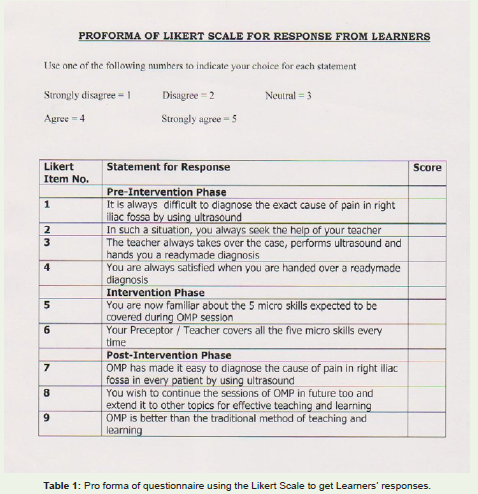
Table 1: Pro forma of questionnaire using the Likert Scale to get Learners’ responses.
In order to further assess the effectiveness of this study, the fourlevelmodel created by Donald Kirkpatrick [10] was also utilised.
Level 1 - Reactions -- Evaluation at this level measures howparticipants in a training programme react to the programme.
Level 2 - Learning -- Evaluation at this level attempts to ascertainthe extent to which students have advanced in skills, knowledge orattitude.
Part C: Included at the state of vaccination, present or absent of edema, diarrhea, pattern of feeding, time of weaning, eye signs, and presence or absence of dermatitis.
Level 3 - Transfer -- This level measures the transfer that occurred in learners’ behaviour due to the training programme.
Level 4 - Results -- Often referred to as “the bottom line,” this level addresses the success of a training programme.
Results
The response of all the residents (n =12) who willingly participated in this study to each Likert item was obtained and is summarised in Table 2. As demonstrated by average score of 4 for Likert item 1; most of the residents agreed that it was difficult for them to diagnose the exact cause of pain inpatients presenting with acute abdomen using ultrasound. In such a situation, the majority of them (8 out of 12) sought the help of their teacher who then took over the case, performed ultrasound himself and handed them a ready-made diagnosis (9 out of 12). This left most of the residents unsatisfied as shown by the reply to Likert item 4 which has an average score of just 2.16. After demonstration of OMP, all the residents became familiar with its 5 steps (Likert item 5; average score of 4.5) and they also agreed to the fact that their teacher covered all 5 steps of OMP each time (Likert item 6; average score of 4.5). Most of the residents agreed that implementation of OMP made it easier for them to diagnose the cause of pain in such cases referred for ultrasound(Likert item 7; average score of 4.3), and wished to continue sessions of OMP in the future with extension into other topics as well (Likert item 8; average score of 4.58) and felt that OMP was better than the traditional methods of teaching and learning (Likert item 9; average score of 4.5).
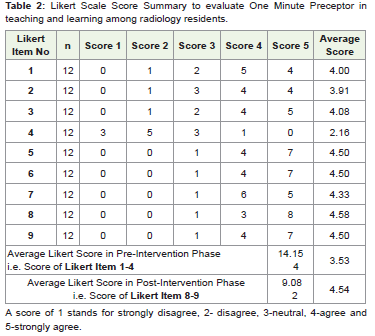
Table 2: Likert Scale Score Summary to evaluate One Minute Preceptor in teaching and learning among radiology residents.
Figure 1 compares as well as demonstrates the improvementin average scores on Likert Scale following the introductionand implementation of OMP by showing a comparison of preintervention(3.5) and post-intervention (4.5) average scores.

Figure 1: Bar diagram showing pre [1] and post [2] intervention Likert scores.
Donald Kirkpatrick`s four-level evaluation model showed thefollowing results:
Level 1 - Reactions -- All 12 residents as well as the single preceptor actively participated in this training programme.
Level 2 - Learning -- As is evident from Likert item responsenumber 1 to 4 [pre-test] having a mean value of 3.5 and item number 8 to 9 [post-test] having a mean value of 4.54, the learners’ levelof learning and confidence in accurate diagnosis has significantlyimproved (p < 0.01).
Level 3 - Transfer -- The preceptor himself saw that the newlyacquired skills, knowledge and attitude have shown a significantpositive change. All the cases were real-life cases on which theresidents performed ultrasound, participating in this programmeduring their individual emergency hours when the preceptor wascalled to opine. Of the 12 cases, 3 were of acute Cholecystitis, 5 wereof appendicitis, 2 were of mesenteric lymphadenitis, 1 was of leftureteric calculus and 1 was of diverticulitis.
Level 4 - Results -- All the learners can now satisfactorily comeout with a definitive cause of pain in patients with acute abdomenwith the use of ultrasound for diagnosis, compared to the pre-projectstatus where the diagnosis was rarely definitive and was more oftenonly speculative.
Possible bias in this programme from the preceptor`s end[teacher] is in interpreting the response as satisfactory (nevertheless,the preceptor tried to be as neutral as is possible for a human beingin this position) and from the resident`s end is in always giving apositive response.
Discussion
Medical residents are supposed to do multiple taskssimultaneously. Apart from learning for their educational goals, theyare also expected to manage patients in a busy setting. It is thereforeappealing if a way can be found to teach individual residents in thebusy clinical setting itself so that the teacher and resident can interact and take care of the patient simultaneously. This type of teachinglearning activity is highly desirable as the teacher can have oneon- one time with residents, directly observe them, monitor patient involvement, and educate them in a relevant, real-life scenario [11]. This ideal approach needs proper planning as the time available withindividual patients and/or with individual residents is limited.
“One Minute Preceptor” (OMP) has emerged as an effectivemodel for teaching in such clinical settings [4]. Within a short span oftime, OMP enables the efficient “shaping” of educational discussionsso that the teacher as well as the student can both benefit [5,12]. The beauty of OMP is that it can be taught in a single one- to two-hourseminar. It focuses on a few teaching behaviors that the residentas well as the teacher can easily perform [4]. So, at the same time,while OMP is being practised, the teacher as well as the resident can“diagnose” the patient and can simultaneously teach the resident byusing the five micro skills of OMP.
As shown in the results of the present study, the use of OMPfor radiology residents in an ambulatory setup, like ultrasoundout-patient department, has positively contributed in achievingits objectives of developing the thought process to reach the exactdiagnosis by utilizing medical history, and clinical examination andproper ultrasound analysis. The ‘commitment part’ encourages theresidents to read more and also increases their contact time andinteraction with the patients. It also helps them to write better reportsand achieve better diagnostic skills.
OMP makes the preceptors aware of the learners’ strong and weakareas of need so that they can focus on those areas and bring out thebest in the learners. OMP has thus emerged as a satisfactory approachand a problem-solving tool in this scenario. It is quite possible thatother educational interventions could have been even more effective,but a comparative study was not carried out.
The first step of getting a commitment from the resident improvesthe resident’s confidence and encourages their analytical and selfexpression skills. The second step in which the preceptor probes the residents’ underlying reasoning enables the residents and preceptor to understand the gaps in the learning process so that they can be appropriately addressed in the third step of giving positive feedback, fourth step of correcting errors in reasoning and in the fifth and final step of teaching general rules which are the key teaching points on that particular topic.
An initial experience with OMP [1] has now enabled andencouraged the preceptor as well as the residents, to use the conceptof OMP in other topics that residents find difficult to master.
OMP has thus paved a way for a fruitful and satisfactory teachinglearning experience for the residents and their teacher that ultimately manifests as an improved diagnosis of the patient`s ailment, which is the prime aim of this speciality.
The limitations of this study are the small sample size (n=12) andthe limited scope, which was restricted to the utility of ultrasound inevaluating patients with acute abdomen. Larger comparative studiesare therefore needed for drawing statistical inferences. Moreover,although it is possible that the significant positive outcome (p < 0.01) on Likert Scale might be due to false response by the residentsto please the faculty, Kirkpatrick`s evaluation method reflects thechanges in their day-to-day approach which cannot be missed by anypreceptor.
Studies have reported that both residents and teachers rate OMPas a more effective model of teaching than traditional methods [3,13].The results of interactive faculty - resident development workshopsfocused on OMP – have shown modest improvements in the quality offaculty feedback delivered in the ambulatory setting [6] and residentteaching skills in the inpatient care setting [3]. The effectiveness of OMP faculty development workshops can be enhanced with theintroduction of highly-scripted cases and standardised learners asit helps participants overcome dissatisfaction with role-playing andprovides increasingly challenging and at the same time authenticclinical teaching scenarios for skills practice [14].
References
- Kachewar SG (2014) A Novel Teaching Technique to Diagnose Cause of Right Iliac Fossa Pain. Journal of The Analgesics 2: 1-5.
- Aagaard E, Teherani A, Irby TM (2004) Effectiveness of the One Minute Preceptor model for diagnosing the patient and the learner: Proof of concept. Acad Med 79: 42-49.
- Furney SL, Orsini AN, Orsetti KE, Stern DT, Gruppen LD (2001) Teaching of One Minute Preceptor, a randomized controlled trial. J Gen Intern Medicine 16: 620-624.
- Neher JO, Gordon KC, Meyer B, Stevens N (1992) A five-step "micro skills" model of clinical teaching. J Am Board Fam Pract 5: 419-424.
- Irby DM, Aagaard E, Teherani A (2004) Teaching points identified by preceptors observing one minute preceptor and traditional preceptor encounters. Acad Med 79: 50-55.
- Salerno SM, O’Malley PG, Pangaro LN, Wheeler GA, Moores LK, et al. (2002) Faculty development seminars based on one minute Preceptor improve feedback in the ambulatory setting. J Gen Intern Medicine 17: 779-787.
- Eckstrom E, Horner L, Bowen JL (2006) Measuring outcomes of one Minute preceptor faculty development workshop. J Gen Intern Medicine 21: 410-414.
- Likert R (1932) A Technique for the Measurement of Attitudes. Archives of Psychology 140: 1-55.
- James C, Perla RJ (2007) Ten Common Misunderstandings, Misconceptions, Persistent Myths and Urban Legends about Likert Scales and Likert Response Formats and their Antidotes. J Social Sciences 3: 106-116.
- Kirkpatrick DL, Kirkpatrick JD (2006) Evaluating Training Programmes: The Four Levels. 3rd ed. San Francisco, CA, USA: Berrett-Koehler Publishers 21-74.
- Ferenchick G, Simpson D, Blackman J, DaRosa D, Dunnington G (1997) Strategies for efficient and effective teaching in the ambulatory care setting. Acad Med 72: 277-280.
- Neher JO, Stevens NG (2003) The One Minute preceptor: shaping the teacher’s conversation: Family Medicine 35: 391-393.
- Teherani A, O'Sullivan P, Aagaard EM, Morrison EH, Irby DM (2007) Student perceptions of the one minute preceptor and traditional preceptor models. Med Teach 29: 323-327.
- Bowen JL, Eckstrom E, Muller M, Haney E (2006) Enhancing the effectiveness of One-Minute Preceptor faculty development workshops. Teach Learn Med 18: 35-41.