Letter to Editor
Chorea in Nonketotic hyperglycemia
Prashant S Naphade1* and Abhishek R Keraliya2
Corresponding author: Prashant S. Naphade, M.D., D.N.B., Fellow in Neuroradiology, Department of CT/MRI, ESIC Hospital, Central road, Andheri east, Mumbai-400093, India,; E-mail: atiarh@yahoo.com
Citation: Naphade PS, Keraliya AR. Chorea in Nonketotic hyperglycemia. Indian J ApplRadiol. 2015;1(1): 101.
Copyright © 2015 Prashant S Naphade et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Applied Radiology | Volume: 1, Issue: 1
Submission: 20/05/2015; Accepted: 29/06/2015; Published: 04/07/2015
Sir,
A 56 year diabetic lady presented with an episode of suddenonset chorea involving right half of body lasting for approximately 30minutes. Neurological examination was unremarkable. Laboratoryexamination revealed high blood glucose levels (346 mg/dl) withabsence of ketone bodies in urine. MRI brain performed 10 dayslater revealed abnormal focal T2/FLAIR hypointense signal inthe left caudate, globus pallidus and putamen with thin rim ofT2 hyperintensity (Figure 1A & B, arrow). These lesions appearhyperintense on T1 weighted images (Figure 1C, arrow). No evidenceof restriction of diffusion was seen on diffusion weighted images.These are classic imaging findings of chorea induced by Nonketotichyperglycemia.
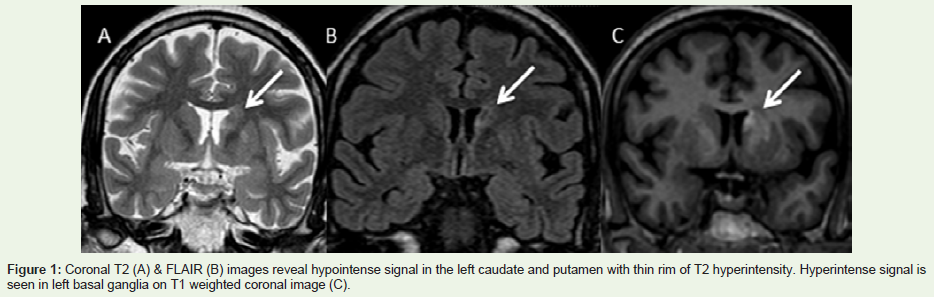
Figure 1: Coronal T2 (A) & FLAIR (B) images reveal hypointense signal in the left caudate and putamen with thin rim of T2 hyperintensity. Hyperintense signal isseen in left basal ganglia on T1 weighted coronal image (C).
Nonketotic hyperglycemia commonly occurs in elderly patientswith non-insulin dependent uncontrolled diabetes mellitus.Presenting features varies from focal seizures, focal neurological deficit, chorea and hyperosmolar coma in severe cases. In acute phase,Nonketotic hyperglycemia can be confused with ischemic stroke onMRI due to restriction of diffusion. Hypointensity on T2 weightedimages and hyperintensity on T1 weighted images can be due tomicrocalcifications or petechial hemorrhages [1]. Resolution of theseMRI findings correlates with disappearance of chorea [2]. Treatmentis directed towards normalization of blood glucose with intravenousfluids and insulin therapy.
References
- Wintermark M, Fischbein NJ, Mukherjee P, Yuh EL, Dillon WP. Unilateralputaminal CT, MR, and diffusion abnormalities secondary to nonketotichyperglycemia in the setting of acute neurologic symptoms mimicking stroke. AJNR Am J Neuroradiol. 1986; 25:975-976.
- Oh SH, Lee KY, Im JH, Lee MS. Chorea associated with non-ketotic hyperglycemia and hyperintensity basal ganglia lesion on T1-weighted brain MRI study: a meta-analysis of 53 cases including four present cases. J NeurolSci. 2002; 200:57-62.