Research Article
Awareness, Perception, and Use of Front of- Pack Nutrition Labels (FOPNLs) among Parents/ Guardians of School Children: A Mixed-Method Study in South Delhi
Sharma S1*, Chatterjee K1, Samanta I2, Mahajan S3 and Misra A4
1Department of Community Medicine, Armed Forces Medical College, Pune, Maharashtra, India
2Station Health Organisation (Large), Delhi Cantonment, Delhi, India
3Station Health Organisation (Large), Shakurbasti, Delhi, India
4Department of Hospital Administration, Armed Forces Medical College, Pune, Maharashtra, India
2Station Health Organisation (Large), Delhi Cantonment, Delhi, India
3Station Health Organisation (Large), Shakurbasti, Delhi, India
4Department of Hospital Administration, Armed Forces Medical College, Pune, Maharashtra, India
*Corresponding author: Dr. Sakshi Sharma, Department of Community Medicine, Armed Forces Medical College, Pune, Maharashtra E-mail Id: sakshi99100@gmail.com
Article Information:Submission: 15/08/2025; Accepted: 03/09/2025; Published: 05/09/2025
Copyright: © 2025 Sharma S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Introduction: India has been facing a public health crisis of Non-Communicable Diseases (NCDs). Front-of-Pack Nutrition Labels (FoPNLs) are a crucial public health strategy that empowers consumers to make healthier and informed dietary choices. Despite national efforts to standardize labelling in India, little is known about how parents, who are the primary decision-makers for children’s diets, perceive and use these labels..
Aims and Objectives: The study aims to assess the awareness, perception, and use of FOPNLs among parents/ Guardians of school children in South Delhi and explore the contextual factors that influence their attitudes and behaviours toward these food labels..
Methodology: 246 parents/ local guardians of school-going children in a public school in South Delhi were interviewed through a structured,.
pre-validated questionnaire and qualitative insights from semi-structured in-depth interviews, to explore deeper attitudes, motivations, and barriers related to FOPNL use. Quantitative data analysis was done using SPSS Ver 26, and qualitative data analysis using thematic coding..
Results: Quantitative findings revealed that 47.3% of participants were aware of the Front-of-Pack Nutrition Labels (FOPNLs). Education level and health consciousness were significantly associated with higher FOPNL use (p < 0.05). Qualitative findings revealed themes such as “Decoding of labels”, “mistrust of packaged food”, and “children’s food preferences overriding label information”. Results highlight gaps in awareness and understanding, with implications for future health literacy interventions and public sensitization.
Conclusions: The awareness of FOPNLs among parents/ local guardians in South Delhi is average and actual usage in daily food purchasing decisions remains low. The study highlights the need for targeted nutrition education campaigns to improve food literacy and promote healthier dietary choices for children.
Aims and Objectives: The study aims to assess the awareness, perception, and use of FOPNLs among parents/ Guardians of school children in South Delhi and explore the contextual factors that influence their attitudes and behaviours toward these food labels..
Methodology: 246 parents/ local guardians of school-going children in a public school in South Delhi were interviewed through a structured,.
pre-validated questionnaire and qualitative insights from semi-structured in-depth interviews, to explore deeper attitudes, motivations, and barriers related to FOPNL use. Quantitative data analysis was done using SPSS Ver 26, and qualitative data analysis using thematic coding..
Results: Quantitative findings revealed that 47.3% of participants were aware of the Front-of-Pack Nutrition Labels (FOPNLs). Education level and health consciousness were significantly associated with higher FOPNL use (p < 0.05). Qualitative findings revealed themes such as “Decoding of labels”, “mistrust of packaged food”, and “children’s food preferences overriding label information”. Results highlight gaps in awareness and understanding, with implications for future health literacy interventions and public sensitization.
Conclusions: The awareness of FOPNLs among parents/ local guardians in South Delhi is average and actual usage in daily food purchasing decisions remains low. The study highlights the need for targeted nutrition education campaigns to improve food literacy and promote healthier dietary choices for children.
Keywords:Front-Of-Pack Nutrition Labels (Fopnls); Nutritional Education; School Children; Mixed Method Study, South Delhi
Introduction
India is facing a public health crisis of Non-Communicable
Diseases (NCDs) like obesity, diabetes, cancers, hypertension, cardiac
diseases, renal disease, and mental health conditions. It is estimated
that nearly 5.8 million people die from NCDs every year out of total
deaths of about 9 million, contributing to about 60% of annual deaths
out of the total 9 million deaths. [1] Ultra-processed unhealthy food/
drink products (UPFs) are significantly associated with high risks
of NCDs and all-cause mortality. [2] Unhealthy diets account for
56.4% of the total disease burden in the country, as per the ICMRNIN
Dietary Guidelines for Indians. [3] Childhood obesity strongly
predicts adult obesity and carries considerable health and economic
consequences for individuals as well as society. [4,5]
The Comprehensive National Nutrition Survey (CNNS) 2016
reveals that more than half of the 5–19-year-olds exhibit biomarkers
of NCDs, which are increasingly linked to dietary risk factors. There
is a rising trend of NCDs, which is attributed mostly to urbanization,
sedentary lifestyles, calorie-dense foods, and marketing of ultraprocessed
foods have intensified poor nutritional habits, particularly
among children [6,7].
In response to these concerns, Front-of-Pack Nutrition Labels
(FoPNLs) are an evidence-based intervention endorsed by WHO and
the Food Safety and Standards Authority of India (FSSAI) to promote
informed food choices. [8] FOPNLs aim to provide simplified, easily
visible, and interpretive nutrition information to consumers at the
point of purchase. [9,10] They serve as a behavioral “nudge” to
guide healthier food choices and promote long-term shifts in dietary
patterns. [11,12]
There are three components of Nutritional Labelling: nutrient
declarations, nutrition and health claims, and supplementary nutrition
information. There are two types of understanding: subjective and
objective comprehension. The former refers to the customer’s capacity
to interpret the FoPNL information as intended by its creators. [13]
whereas the latter involves analysing the labelling information as
intended by its designers [14]. Many countries, including India, have
mandated the declaration of nutrition information on labels (FSSAI,
2011) [15]. The supplementary nutrition information is referred to
as Front of Pack Nutrition Labelling (FOPNL). FOPNL could be
one of the several strategic communication methods that are being
implemented to generate awareness and motivate consumers to make
healthy choices. [16,17] In India, FSSAI certification is mandatory for
all packaged food products, ensuring safety and labelling compliance.
In comparison, the ISI mark (BIS) is primarily used for non-food
items, whereas Agmark is a voluntary quality certification for
agricultural products.
In addition to enhancing understanding of nutritional
information, FOPNL promotes healthier food choices and drives
the food industry to reformulate products toward more balanced
nutritional profiles. [18,19] Thus, it may help reduce the risk of obesity
and non-communicable diseases. FOPNLs are cost-effective means to
empower individuals in making healthier food choices at the point of
purchase and hence improve dietary intake at the population level.
[20]
However, parental understanding, who are key decisionmakers
and most commonly engage with FOPNLs for children’s
diets, remains under investigated. This study aims to fill the gap
by exploring the parental knowledge of FOPNLs among parents of
school-going children in a public school of South Delhi through a
mixed-methods approach.
Operational Definitions:
Front-of-pack nutrition labelling (FOPNL): “A type of
supplementary nutrition information that displays simplified
nutrition details on the front of pre-packaged foods. It may use
symbols/graphics, text, or a combination to convey the overall
nutritional quality of the product and/or key nutrient content
included in the FOPNL.”High fat, sugar, salt (HFSS) food: “A processed food item that
contains high amounts of saturated fat, total sugar, or sodium. The
declared levels of these components are such that the product fails
to meet the criteria of energy (kcal) from total sugar being less than
10% of total energy, or saturated fat less than 10% of total energy, and
sodium less than 1 mg per kcal.” [21]
Objectives::
1. To assess the awareness and use of Front-of-Pack Nutrition
Labels (FOPNLs) among parents/guardians of school
children in South Delhi.2. To identify sociodemographic determinants of awareness and use of FOPNLs.
3. To explore qualitative insights into barriers and facilitators influencing FoPNL understanding.
Methodology
Study Design:
This study adopted a mixed-methods cross-sectional design,
combining quantitative observational study with qualitative
interviews. The rationale for this approach was to capture both the
breadth (through structured data) and depth (through narrative
insights) of awareness, perception, and use of front-of-pack food
labels among parents of school-going children.The study was conducted in two phases.
In Phase 1: A structured, pre-validated questionnaire was administered to 246 participants (parents/ local guardians) of children aged 5 to 18 years old in a public school in South Delhi.
In Phase II: In-depth interviews (IDIs) were conducted with a purposive sample of 12 participants to explore their attitudes, barriers, and preferences regarding FOPNLs. Participants were selected after completion of the quantitative survey to ensure informed reflection during the interview.
In Phase 1: A structured, pre-validated questionnaire was administered to 246 participants (parents/ local guardians) of children aged 5 to 18 years old in a public school in South Delhi.
In Phase II: In-depth interviews (IDIs) were conducted with a purposive sample of 12 participants to explore their attitudes, barriers, and preferences regarding FOPNLs. Participants were selected after completion of the quantitative survey to ensure informed reflection during the interview.
Study Population: Parents/ local guardians of school-going
children (aged 5-18 years) from an urban public school in South
Delhi.
Inclusion Criteria
• Parents/guardians of children aged 5–18 years currently enrolled in the selected school.
• Those willing to provide informed written consent for participation.
Exclusion Criteria
• Parents not available at the time of the conduct of the study.
• Those unwilling or unable to participate due to language barriers or time constraints
• Parents/guardians of children aged 5–18 years currently enrolled in the selected school.
• Those willing to provide informed written consent for participation.
Exclusion Criteria
• Parents not available at the time of the conduct of the study.
• Those unwilling or unable to participate due to language barriers or time constraints
Sample Size:
• Quantitative armAssuming that 20% of participants buying pre-packaged foods read nutrition information on labels, with a 95% confidence level (Z = 1.96) and an absolute precision of 5%, the formula for sample size calculation was applied using the values p = 0.2 (p is the assumed proportion) and q = 0.8 using the Cochran’s formula.
n = Z2(1 -α/2) P (1- P) /d2
This resulted in a final calculated sample size of 246 participants.
• Qualitative arm
12 parents were selected using purposive sampling to participate in in-depth interviews. Participant selection considered diversity in educational status, income level, and awareness of FOPNLs. The sample size for the quantitative component was determined based on practical feasibility, the expected response rate, and the aim of detecting meaningful associations. The principle of thematic saturation guided the selection of the qualitative sample size.
12 parents were selected using purposive sampling to participate in in-depth interviews. Participant selection considered diversity in educational status, income level, and awareness of FOPNLs. The sample size for the quantitative component was determined based on practical feasibility, the expected response rate, and the aim of detecting meaningful associations. The principle of thematic saturation guided the selection of the qualitative sample size.
Sampling Technique
• Quantitative component: A simple random sampling technique was employed, and participants were randomly selected from the school lists • Qualitative component: Purposive sampling was used.
• Quantitative component: A simple random sampling technique was employed, and participants were randomly selected from the school lists • Qualitative component: Purposive sampling was used.
Data Collection Tools:
1. Quantitative Tool: Data was collected by administering the
questionnaire in an interview mode. Participants completed
the instrument in English/ Hindi. A pre-structured,
standardized and pre-validated questionnaire was used to
assess awareness, understanding, and preference related to
various formats of Front-of-Pack Nutrition Labels (FOPNLs)
among parents/ local guardians of school-going children.
The tool was adapted from the ICMR-National Institute of
Nutrition (NIN), Hyderabad, as detailed in the report titled
“Assessing Effectiveness of Front-of-Pack Nutrition Labels in
India” (2023) [22].This questionnaire includes sections evaluating::
Part 1: The first part of the questionnaire collected
sociodemographic details, frequency of consumption of packaged
foods, food label usage habits, and their practice of reading the
nutrition information on the label.Part 2: The second part of the questionnaire assessed the perceptions of the participants on likeability, attractiveness and perceived cognitive workload of the five different formats of the FOPNL tested.
Part 3: The third part of the questionnaire assessed the objective understanding, perceived product healthfulness, purchase intention and willingness to change purchase behaviour of the participants.
2. Qualitative Tool: A qualitative descriptive study was conducted using semi-structured in-depth interviews (IDIs) with a purposively selected subset of parents. An interview guide was developed to explore perceptions of various food labelling formats, Barriers to understanding and usage, Influence of FoPNL on dietary choices and trust in food label information
Data Collection Procedure:
Face to Face-to-face interviews were conducted in a quiet setting,
lasting approximately 30–40 minutes and were conducted in either
Hindi or English, according to the participant’s language preference.
Before initiation, informed consent was obtained from each
participant, and interviews were audio-recorded and subsequently
transcribed verbatim to ensure accuracy. The interview guide
comprised open-ended questions designed to explore participants’
perceptions, experiences, and preferences regarding nutrition labels
on packaged foods.Ethical Considerations: Ethical approval was obtained from
the Institutional Ethics Committee. Written informed consent was
obtained from all participants before data collection and audio
recording. Confidentiality was maintained by anonymizing school
and participant identifiers. Participation was voluntary, and parents
could withdraw at any stage.
Quantitative Data Analysis: Descriptive statistics (frequencies,
percentages, means ± SD) were computed for demographic variables
and responses related to awareness and usage of FoPNL. Bivariate
analyses (Chi-square test) were conducted to explore associations
between demographic characteristics (e.g., education level, income)
and outcomes. For ordinal or non-normally distributed continuous
variables, non-parametric tests such as the Kruskal–Walli’s test were
applied. Data was collated and cleaned using MS Excel and was
analysed using SPSS Version 26(IBM Corp., Armonk, NY, USA).
Qualitative Data Analysis: Manual coding of interview
transcripts was done and the thematic analysis framework by Braun
and Clarke (2006) was followed. [23] Initial coding was done line-byline,
and codes were grouped into categories and overarching themes.
Results
Participant Characteristics:
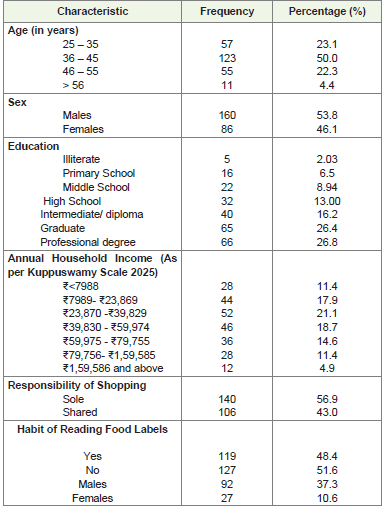
The mean age of the participants was 37.17 ± 6.51 years, with an
average height of 171.55 ± 8.27 cm, and a mean weight of 77.62 ±
13.00 kg. Most respondents were married (81.3%) and responsible for
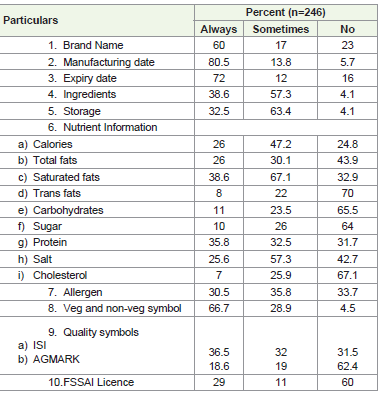
sole (56.9%) or shared (43.1%) household grocery shopping [Table 1].Awareness and Use of Food Labels: As depicted in [Table 2], most participants reported checking basic details such as the manufacturing date (80.5%), expiry date (72%), and veg/nonveg symbol (66.7%), while fewer consistently checked nutrient information. Only around one-fourth examined calories (26%), total fat (26%), salt (25.6%), and protein (35.8%), with very few looking at trans fats (8%), cholesterol (7%), or carbohydrates (11%). Regulatory details like FSSAI license (29%), AGMARK (18.6%), and ISI mark (36.5%) were also infrequently checked. Overall, participants prioritized basic product details over critical nutritional and safety information.
A majority of males, 37.3% reported reading food labels, compared
to only 10.6% females [Table 2]. Interestingly, more females reported
not reading labels than those who did, whereas among males, the
reverse was true, with more engaging in the habit. This suggests that
males in this group are more likely than females to read food labels,
which may reflect differences in health awareness, purchasing roles,
or nutrition education between genders [Figure 1].
28.9 % of participants don’t check the quality symbol on the
packaged food items, whereas 36.5% of the participants check the ISI
mark on the food labels, 18.6% check the AGMARK label and only
15.8% check the FSSAI license [Figure 2].
Participants were mostly unfamiliar with the Nutri-star or traffic light labelling system for food products. Among males, nearly threefourths (72%) were unaware, compared to 59% of females. Awareness was relatively higher among females (41%) than among males (28%).
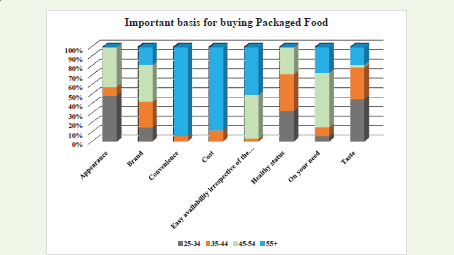
Figure 3 illustrates age-related differences in the basis for purchasing packaged foods. Younger adults (25–34 years) prioritized sensory factors such as appearance (55%) and taste (50%), while middle-aged participants (35-44 and 45-54 years) more often considered health status and brand. In contrast, older adults (55+ years) placed the greatest emphasis on convenience, cost, and easy availability. These findings suggest that while younger consumers are guided largely by sensory appeal, middle-aged adults balance brand and health considerations, and older adults rely primarily on practical factors such as accessibility and affordability.
Participants were mostly unfamiliar with the Nutri-star or traffic light labelling system for food products. Among males, nearly threefourths (72%) were unaware, compared to 59% of females. Awareness was relatively higher among females (41%) than among males (28%).
Figure 3 illustrates age-related differences in the basis for purchasing packaged foods. Younger adults (25–34 years) prioritized sensory factors such as appearance (55%) and taste (50%), while middle-aged participants (35-44 and 45-54 years) more often considered health status and brand. In contrast, older adults (55+ years) placed the greatest emphasis on convenience, cost, and easy availability. These findings suggest that while younger consumers are guided largely by sensory appeal, middle-aged adults balance brand and health considerations, and older adults rely primarily on practical factors such as accessibility and affordability.
Association between Educational Qualification, Income and Habit of Reading Food Labels:
Among participants with a professional degree, 62.1% reported
reading food labels (n=82), whereas among those with graduate-level
education, only 12.7% (n=9) reported this habit. For participants with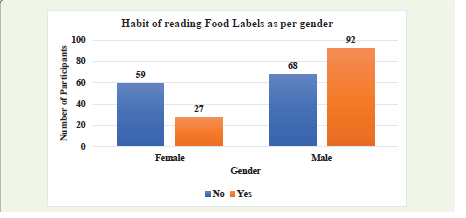
intermediate/diploma and high school education, the proportions
were 27.6% (n=8) and 21.4% (n=3) respectively. This suggests that
the tendency to read food labels increased with higher educational
attainment. A significant association was found between educational
qualification and the habit of reading food labels (χ² = 80.17, df = 9,
p < 0.001). Participants with higher education, especially those with
professional degrees, were more likely to read food labels compared
to those with lower educational levels. This highlights the role of
education in influencing health-conscious behaviours.
Individuals in the highest income group (₹1,59,586) are more
likely to read food labels compared to other groups, suggesting greater
health awareness and purchasing power in this category. In contrast,
the lowest income group (₹<7,988) shows minimal engagement with
label reading
Habit of checking Salt and Sugar content on Food Labels:
Only 20.3% of participants reported always checking salt
content on food labels, while 30.5% did so occasionally. More than
half (49.2%) never checked salt information, indicating limited
engagement with this nutrient despite its known association with
hypertension and other non-communicable diseases. The Kruskal-
Wallis test (p = 0.336) revealed a statistically significant difference
between the “never,” “sometimes,” and “always” groups, indicating
that salt label–reading behaviour was associated with meaningful
differences in body weight in this sample.Similarly, for sugars, only 18.7% of participants reported always
checking sugar content on food labels, while 32.4% did so occasionally
and 48.9% never checked sugar information, highlighting a gap in
consumer attention despite the well-established role of high sugar
intake in obesity and metabolic disorders. The Kruskal–Wallis test
(p = 0.028) revealed a statistically significant difference between the
“never,” “sometimes,” and “always” groups, indicating that sugar
label–reading behaviour was associated with meaningful differences
in body weight in this sample.
Association between Weight and Checking of Nutrition Information (Sugar):
A cross-tabulation of weight and frequency of checking nutrition
information for sugar revealed distinct behavioral patterns. Only
3.7% of participants reported always checking labels, while the
majority either never (41.9%), sometimes (26.8%), or rarely (27.6%)
engaged in this practice. Participants with lower body weights (<70
kg) were more likely to report “always” checking labels, whereas
those with higher body weights (≥80 kg) overwhelmingly fell into the
“never,” “sometimes,” or “rarely” categories, with striking uniformity
seen at 83 kg (all never), 85 kg (all sometimes), and 86 kg (all rarely).
The mean weight among “always” checkers was 65.3 kg compared
to 77–80 kg in the other groups, and the difference was statistically
significant (Kruskal–Wallis χ² = 15.44, p = 0.0015). These findings
suggest that consistent engagement with nutrition labels, particularly
for sugar content, may be associated with healthier body weight,
whereas lack of such behaviour is more prevalent among heavier
individuals.Association between Body Weight and Habit of Reading Food Labels:
A total of 246 participants were assessed for the association
between body weight and food label–reading habits. Individuals in
the normal weight range were more likely to read food labels, whereas
those in higher weight categories (≥85 kg) predominantly did not,
indicating a negative association between increasing body weight
and label-reading behaviour. This trend may indicate either a lack
of awareness or motivation toward nutrition-conscious behaviours
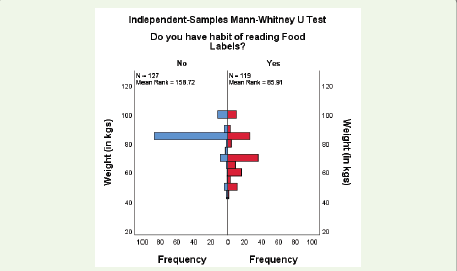
among individuals with higher body mass.The association between food label reading habits and body weight was assessed using the Mann–Whitney U test [Figure 4]. Participants who reported reading food labels (n = 119, mean rank =
85.91) had significantly lower weights compared to those who did not
read food labels (n = 127, mean rank = 158.72), indicating that label
readers were generally lighter in weight. This suggests that the habit of
reading nutrition labels is associated with healthier weight outcomes.
A majority of both males and females reported unfamiliarity, with the proportion being higher among males, indicating low overall awareness of front-of-pack labelling systems across genders, with a slightly higher level of awareness among males [Figure 5].
A majority of both males and females reported unfamiliarity, with the proportion being higher among males, indicating low overall awareness of front-of-pack labelling systems across genders, with a slightly higher level of awareness among males [Figure 5].
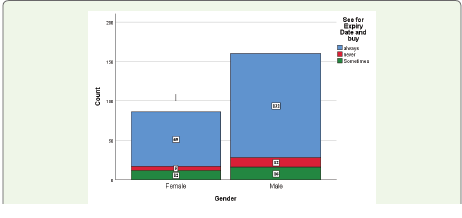
Gender-wise comparisons of checking expiry date on packaged food:
Most participants reported always checking expiry dates before
purchasing food products, with this habit being more prevalent
among 65.4% of males and 52.7% of females following this practice.
Only a small fraction (4.5% males and 6.9% females) reported never
checking expiry dates, indicating generally good consumer awareness
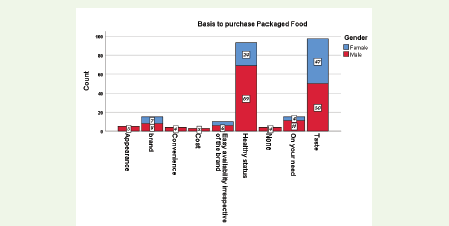
across genders [Figure 6].Among male respondents, the most common purchase drivers for packaged food were health status (34.5%), followed by taste (25.0%). In contrast, female respondents most frequently cited taste (23.5%), followed by health status (12.0%) [Figure 7]. Other factors, such as appearance, brand, convenience, cost, and easy availability, were reported less frequently by both genders. A statistically significant association was observed between gender and the basis for purchase of packaged food (χ² = 24.36, df = 6, p < 0.001).
Association between Marital Status and Habit of Reading Food Labels:
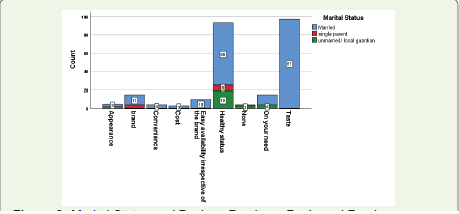
Across marital status groups, the most frequently reported basis
for purchasing packaged food was taste among married respondents
(49.0%), followed by health status (46.5%). For single parents, health
status (12.0%) was the predominant reason, while unmarried/local
guardian respondents most frequently cited health status (10.5%).
Other factors, such as brand preference, appearance, convenience,
and cost, were reported much less frequently across all groups. A
statistically significant association was found between marital status
and basis for purchase (χ² = 31.42, df = 6, p < 0.001), indicating that
purchase motivations differ by marital status [Figure 8].Association between Comorbidities and Habit of Reading Food Labels:
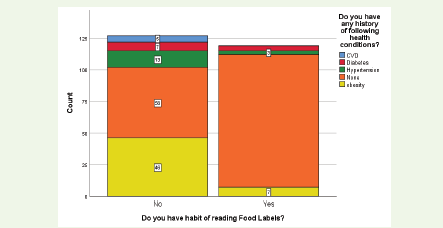
Among the 246 participants, the majority (65.4%) reported no
history of cardiovascular disease (CVD), diabetes, hypertension, or
obesity. Obesity (21.5%), hypertension (6.5%), diabetes (4.5%), and
CVD (2.0%) were the most commonly reported conditions among
those with a medical history. Reading of food labels was more
common among participants with no history of these conditions
(65.2%) compared to those with CVD, obesity (13.2%), hypertension
(18.8%), or diabetes (36.4%). Overall, 48.4% of participants reported
reading food labels, indicating a moderate level of engagement with
nutritional information. Notably, individuals without chronic health
conditions had the highest proportion of label-reading behavior,
while those with obesity and CVD were the least likely to read labels
[Figure 9].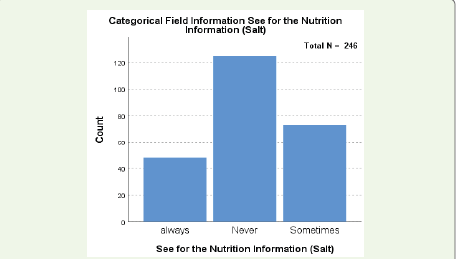
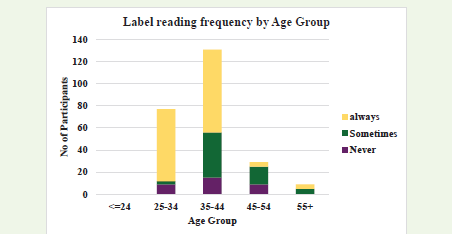
Binary logistic regression analysis was performed with the habit
of reading food labels (Yes/No) as the dependent variable and age (in
years) as the independent variable. The model indicated that age was
not a statistically significant predictor of the habit (β = 0.032, OR =
1.03, 95% CI: 0.96–1.09, p = 0.375. This suggests that the likelihood of
reading food labels does not significantly change with increasing age
in the study population.
Qualitative Findings:
Thematic analysis of 12 in-depth interviews revealed four
overarching themes with associated sub-themes. These insights
provide explanatory depth to the quantitative findings, highlighting
why awareness and usage of FOPNLs remain suboptimal despite
moderate exposure to packaged foods.1. Visual Clarity vs. Difficulty Decoding:
Sub-themes:
i. Font and Layout Issues – Small print, dense text, and placement at the bottom or side of the pack limited visibility.
ii. Symbol Interpretation Gaps – Colour codes and icons were often misunderstood or overlooked.
“Sometimes I see the label, but I don’t know what the figures mean for my child’s health.” (Parent, Male, 42)
“I thought the red circle was just a design, I didn’t know it meant high sugar.” (Parent, Female, 39)
2. Trust vs. Skepticism::
Sub-themes:i. Brand Reliance – Well-known brands were assumed to be healthier.
ii. Perceived Manipulation – Some participants believed labels are intentionally misleading.
“If the brand is good, the food is good – I don’t need to read the label. We feel good brands sell good food.” (Parent, Female, 34) “Companies will never show the bad things clearly, so why bother reading?” (Guardian, Male, 56)
3. Time Constraints::
Sub-themes:i. Shopping in a Rush – Limited time to compare products.
ii. Competing Priorities – Price, availability, and taste often take precedence.
“I’m always in a hurry, so I just pick what we always buy. I miss checking the labels.” (Parent, Male, 36)
“I check the expiry date, vegetarian and non-vegetarian symbol and move on; I don’t have time for the rest.” (Parent, Female, 41)
4. Child-Centric Decision-Making::
Sub-themes:i. Peer Influence on Children – Children request items seen in advertisements or with peers.
ii. Parental Compromise – Health concerns are sometimes secondary to avoiding conflict.
“If my kid likes it, I don’t think too much about sugar or fat. What children see among peers, they ask for it” (Parent, Female, 34) “Sometimes I know it’s not healthy, but saying no is a bigger fight. My child becomes very fussy and I don’t have any option but to give him what he desires to eat. It becomes very difficult as a parent” (Parent, Male, 39)
These themes highlight that barriers to FOPNL use are not solely cognitive (lack of awareness/understanding) but also behavioural (time and purchasing habits), and social (child and family influence). Addressing these factors through targeted parental education and integration into school and community nutrition programmes could enhance FOPNL effectiveness and support healthier dietary choices.
Discussion
Findings from both quantitative and qualitative arms of the
study demonstrate a considerable gap in parental awareness and
interpretation of Front-of-Pack Nutrition Labels (FoPNLs). Despite
frequent exposure to packaged foods, most parents lacked sufficient
understanding of label formats and their health implications.
Educational level and health literacy emerged as significant
determinants of label use, while external factors such as time
constraints, brand loyalty, and children’s taste preferences frequently
overrode nutritional considerations. These results highlight a
complex interplay between individual capacity, contextual factors,
and marketing influences in shaping parental food choices.
This finding is consistent with prior literature, which suggests that health literacy and educational background are critical in influencing health-related behaviours such as interpreting nutrition labels and making healthier dietary decisions. Studies from India and other low- and middle-income countries (LMICs) have similarly reported that individuals with higher education are more likely to engage with nutrition information, while those with lower literacy tend to rely on brand recognition, pricing, or taste preferences. A study by Sudershan et al has revealed similar findings such as a positive association was found between education level and checking various aspects of food labels. Nutrient information on labels was not often read because most consumers either lacked nutrition knowledge or found the information too technical to understand. The majority looked only for the manufacturing date or expiry/best before date and the findings are consistent with our study. Taste, quality, convenience and ease of use are the main reasons for buying pre-packaged foods. [24] A study by Subbaram et al. revealed low awareness’ for food standards among adolescent girls [25]
The qualitative findings of this study, particularly the themes of trust versus skepticism and child-centric decision-making, echo global evidence that consumer skepticism toward food industry practices and children’s strong influence on household food purchases act as barriers to label effectiveness.
Moreover, the persistence of time constraints and competing priorities reflects a broader behavioral challenge, where convenience and cost often outweigh health concerns. This suggests that providing nutritional information alone may be insufficient unless accompanied by strategies to increase consumer motivation and simplify decision making. The findings reveal that participants predominantly focused on basic product details such as manufacturing and expiry dates, while nutritional components and regulatory symbols were largely overlooked. [26] The low engagement with critical markers like salt, fat, and trans-fat is concerning, given the rising burden of lifestyle related diseases such as hypertension, obesity, and cardiovascular illnesses. [27] Another study by the same author among mothers depicts that the Anganwadi Centres can be the focal points for imparting food safety education to the mothers [28].
Overall, these findings underscore the urgent need for multipronged interventions that address not only individual-level knowledge gaps but also structural and contextual barriers. School based parental sensitization, mass media campaigns, and stricter regulatory policies mandating standardized, easy-to-interpret FoPNLs could bridge the knowledge–practice gap.[29] Furthermore, culturally tailored awareness strategies, particularly for populations with lower educational attainment, may enhance the reach and effectiveness of interventions.
This finding is consistent with prior literature, which suggests that health literacy and educational background are critical in influencing health-related behaviours such as interpreting nutrition labels and making healthier dietary decisions. Studies from India and other low- and middle-income countries (LMICs) have similarly reported that individuals with higher education are more likely to engage with nutrition information, while those with lower literacy tend to rely on brand recognition, pricing, or taste preferences. A study by Sudershan et al has revealed similar findings such as a positive association was found between education level and checking various aspects of food labels. Nutrient information on labels was not often read because most consumers either lacked nutrition knowledge or found the information too technical to understand. The majority looked only for the manufacturing date or expiry/best before date and the findings are consistent with our study. Taste, quality, convenience and ease of use are the main reasons for buying pre-packaged foods. [24] A study by Subbaram et al. revealed low awareness’ for food standards among adolescent girls [25]
The qualitative findings of this study, particularly the themes of trust versus skepticism and child-centric decision-making, echo global evidence that consumer skepticism toward food industry practices and children’s strong influence on household food purchases act as barriers to label effectiveness.
Moreover, the persistence of time constraints and competing priorities reflects a broader behavioral challenge, where convenience and cost often outweigh health concerns. This suggests that providing nutritional information alone may be insufficient unless accompanied by strategies to increase consumer motivation and simplify decision making. The findings reveal that participants predominantly focused on basic product details such as manufacturing and expiry dates, while nutritional components and regulatory symbols were largely overlooked. [26] The low engagement with critical markers like salt, fat, and trans-fat is concerning, given the rising burden of lifestyle related diseases such as hypertension, obesity, and cardiovascular illnesses. [27] Another study by the same author among mothers depicts that the Anganwadi Centres can be the focal points for imparting food safety education to the mothers [28].
Overall, these findings underscore the urgent need for multipronged interventions that address not only individual-level knowledge gaps but also structural and contextual barriers. School based parental sensitization, mass media campaigns, and stricter regulatory policies mandating standardized, easy-to-interpret FoPNLs could bridge the knowledge–practice gap.[29] Furthermore, culturally tailored awareness strategies, particularly for populations with lower educational attainment, may enhance the reach and effectiveness of interventions.
Conclusion
Parental understanding and utilization of FoPNLs remain low
despite moderate exposure to packaged foods. The study highlights
that education, health literacy, and competing household priorities
strongly influence parental engagement with nutritional labelling.
To improve the effectiveness of FoPNLs, multi-level strategies are
required.
Recommendations
i. Label Literacy Programs: Strengthening label literacy
through community-based and digital educational initiatives
on reading and interpreting food labels. Integration of
modules into school curricula is critical.
ii. Targeted Awareness for Primary Grocery Buyers By focusing interventions on household grocery decision makers, particularly married individuals and women, who demonstrate higher engagement with labels. Implement instore nudges, shelf talkers, and point-of-sale campaigns in supermarkets and local retail outlets.
iii. Focus on Low-Income and Less Educated Groups: Inclusion of label awareness in health camps, community nutrition programs, and Anganwadi services. Use of pictorial, videobased, and interactive materials to explain nutritional quality. Training of community health workers to deliver tailored messages.
iv. Integrate Label Education with Nutrition Counselling: Combining BMI screening with personalized label interpretation sessions helps individuals understand the link between food choices and health outcomes. Promotion of mobile applications that integrate diet tracking with label education.
v. Leverage Digital Media for Behaviour Change: Utilization of social media platforms to disseminate short, engaging content (e.g., reels, infographics, interactive quizzes). Partnering with influencers, healthcare professionals, and educators to debunk myths and promote informed food choices.
vi. School and Youth-Focused Interventions: Conduct of school-based workshops on label reading under the Central Board of Secondary Education (CBSE) ‘s upcoming health initiatives.
vii. Policy-Level Recommendations: Encouragement of educational boards (CBSE/ICSE) to integrate label-reading modules into health education curricula.
ii. Targeted Awareness for Primary Grocery Buyers By focusing interventions on household grocery decision makers, particularly married individuals and women, who demonstrate higher engagement with labels. Implement instore nudges, shelf talkers, and point-of-sale campaigns in supermarkets and local retail outlets.
iii. Focus on Low-Income and Less Educated Groups: Inclusion of label awareness in health camps, community nutrition programs, and Anganwadi services. Use of pictorial, videobased, and interactive materials to explain nutritional quality. Training of community health workers to deliver tailored messages.
iv. Integrate Label Education with Nutrition Counselling: Combining BMI screening with personalized label interpretation sessions helps individuals understand the link between food choices and health outcomes. Promotion of mobile applications that integrate diet tracking with label education.
v. Leverage Digital Media for Behaviour Change: Utilization of social media platforms to disseminate short, engaging content (e.g., reels, infographics, interactive quizzes). Partnering with influencers, healthcare professionals, and educators to debunk myths and promote informed food choices.
vi. School and Youth-Focused Interventions: Conduct of school-based workshops on label reading under the Central Board of Secondary Education (CBSE) ‘s upcoming health initiatives.
vii. Policy-Level Recommendations: Encouragement of educational boards (CBSE/ICSE) to integrate label-reading modules into health education curricula.
Limitations
The study has certain limitations, the study was conducted
in an urban setting, which may limit the generalizability of the
findings. Responses were self-reported, subject to recall and social
desirability bias. Furthermore, the study did not explore the longterm
behavioural impact of label reading on actual dietary patterns
and health outcomes. Future research employing longitudinal study
design is recommended to better understand the causal pathways
and to assess the effectiveness of food labelling in influencing dietary
behaviour and improving public health outcomes.
Conflict of Interest
The authors have none to declare.
References
Citation
Sharma S, Chatterjee K, Samanta I, Mahajan S, Misra A. Awareness, Perception, and Use of Front-of-Pack Nutrition Labels (FOPNLs) among Parents/ Guardians of School Children: A Mixed-Method Study in South Delhi. Indian J Nutri. 2025;12(2): 325.