Research Article
Knowledge, Attitudes, and Practices in Nutrition Counselling: A Survey Analysis among Health Consultants
Basu D1, Ghosh S2, Kumar S3, Sinhababu S4 and Singh N5*
1Medical Director, METTA Care Clinic, Kolkata, India.
2Chief Clinical Coordinator, METTA Care Clinic, Kolkata, India.
3Director & Consultant Diabetologist, Dr Surajeet Patra’s Diabetes Clinic, Bhubaneswar, Odisha, India.
4Consultant Diabetologist, Simlapal, Bankura, West Bengal, India.
5Clinical Dietitian, Oncoheal, Pune, India.
2Chief Clinical Coordinator, METTA Care Clinic, Kolkata, India.
3Director & Consultant Diabetologist, Dr Surajeet Patra’s Diabetes Clinic, Bhubaneswar, Odisha, India.
4Consultant Diabetologist, Simlapal, Bankura, West Bengal, India.
5Clinical Dietitian, Oncoheal, Pune, India.
*Corresponding author:Nidhi Singh, Department of Clinical Dietitian, Oncoheal, Pune, India. E-mail Id:nidhisingh295@gmail.com
Article Information:Submission: 04/04/2025; Accepted: 12/05/2025; Published: 15/05/2025
Copyright: © 2025 Basu D, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Chronic respiratory conditions (asthma, COPD), cancer, diabetes, and cardiovascular conditions (stroke, respiratory failures) are all included in the broad category of diseases known as non-communicable diseases (NCDs), which represent a risk of increasing the burden of disease in adults and the elderly. The majority of NCDs worldwide are primarily caused by unhealthy diets and the malnutrition that results from them. A healthy diet is crucial for preventing noncommunicable diseases (NCDs). On the other hand, unhealthy lifestyle choices, such as smoking, drinking, sleeping poorly, not exercising, experiencing stress, being around pollutants, and not eating enough, can lead to metabolic changes that might cause noncommunicable diseases. Patients frequently receive health information from primary care physicians (PCPs) and health experts. As a result, general practitioners can positively impact their patient’s behavior and lifestyle choices. An overview of the current state of nutritional care and nutritional counselling in health, as well as obstacles to nutritional counselling, are intended to be given through this study. The study examined health consultants’ knowledge, attitudes, and practice of nutrition advice using a
standardized survey. The survey’s findings emphasize the need for a more standardized and reliable approach to nutrition counselling in healthcare settings. In order to make sound nutrition recommendations, primary care physicians and other healthcare professionals must possess the necessary training, resources, and expertise. Primary care physicians (PCPs) can prevent the onset of lifestyle-related illnesses by including nutrition into patient treatment, which will ultimately improve public health outcomes and reduce healthcare expenditures.
Introduction
Globally, the prevalence of diseases linked to poor nutrition,
especially its consequences, is rising for people of all ages and
socioeconomic backgrounds.[1]non-communicable diseases
(NCDs) are a huge group of illnesses that comprise chronic
respiratory illnesses (asthma, COPD), malignant growth,
diabetes, and cardiovascular ailments (including stroke and
respiratory failures).[2] There was a possible risk of an increase
in the burden of diseases among adults and the elderly due to the
epidemiological transition from communicable to NCD.[3,4,5]
A major concern regarding the double expansion of chronic diseases
(living with a chronic condition from early life till death) in India
has also been raised by the reduction of healthy years brought on by
the early onset of diseases, particularly among middle-aged adults.
Chronic diseases are more common in low- and middle-income
nations, where they cause both health and financial losses as individuals
age. Though there is little data in the Indian context, estimates of the
age at which chronic disease first manifests offer support for policy
action.[6] Diet, sometimes considered a lifestyle factor, is associated
with obesity, cardiovascular disease, hypertension, stroke, type 2
diabetes, metabolic syndrome, several cancers, and possibly some
neurological conditions. Additionally, the presence of one disease
often contributes to the emergence of another. For example, obesity
or excess body weight/fat is a risk factor for conditions like type 2
diabetes, hypertension, metabolic syndrome, and a number of
cancers, among others.[7]
Furthermore, when a medical disease does exist, it frequently
plays a role in the development of additional medical conditions.
For example, obesity or excess body weight/fat is a risk factor for
a number of conditions, including metabolic syndrome, type 2
diabetes, hypertension, and some types of cancer. The impact of
nutrition on disease risk and/or on certain disease risk factors may
at times be assessed by studies that incorporate changes to “usual”
eating practices. More recently, the focus of dietary guidelines in
many nations has shifted from specific nutrient intake and disease
risk to overall dietary patterns. However, it is commonly known that
a lack of certain nutrients or a state of inadequate nutrition can lead
to the onset of diseases and/or health issues.[8]
The majority of NCDs worldwide are caused by unhealthy diets
and the malnutrition that results from them. Research that uses
changes to “usual” dietary practices is occasionally utilized to assess
how food affects disease risk and/or particular disease risk variables.
Many chronic diseases can be prevented with dietary changes, but
once a problem has set in, it is frequently necessary to alter a person’s
regular diet to help manage the illness or its symptoms. More recently,
the focus of dietary guidelines in many nations has shifted from
specific nutrient intake and disease risk to overall dietary patterns.
Disease management must involve the use of dietary supplements in
addition to the function that dietary changes play in treating illness
or its symptoms.[8,9]
A comprehensive treatment continuum must take into account
the impact of oral nutritional supplements on lowering the prevalence
of sarcopenia and malnutrition in people with diabetes/prediabetes,
obesity, recovering critical care patients, and cancer patients.
People with chronic diseases or NCDs can benefit from a variety of
oral nutritional products available on the market. Research on the
efficacy of numerous nutraceuticals aimed at disease prevention and
treatment is also booming in the scientific literature. This justifies
the need to understand the “right choice” in order to advance our
understanding of diet and nutrition support for these conditions. We
also need to take appropriate steps to assist healthcare professionals
in educating their patients and assisting them in adopting healthy
eating habits.[10]
The prevention of NCDs is largely dependent on appropriate diet.
An effective strategy to stop NCDs from starting is the Mediterranean
diet, which is defined by a high intake of fruits, vegetables, grains,
legumes, and fish; a moderate intake of dairy products and eggs;
and a low intake of animal fats and red meat. Conversely, a poor
lifestyle—which includes smoking, alcoholism, poor sleep, physical
inactivity, psychological stress, environmental pollution, and
inadequate nutrition—contributes to metabolic alterations that may
initiate NCDs.[8]With the International Diabetes Federation (IDF)
president, Prof. Peter Schwarz, recently introducing the METTA
Dāna Foundation’s (MDF) slogan, “screen for NCD by Twenty,
Add Healthy years, a Plenty,” to a global audience in front of the
renowned Prof. A K Azad Khan, the IDF SEA region chair, we take on
the unique task of identifying the Knowledge, Attitude, and Practices
(KAP) gap in “Diet and NCD” where we see a huge potential to change
the environment of the most ill people in our nation and the entire
world.[11] Any medical treatment intended to improve a patient’s
eating habits and, consequently, health outcomes—especially in
NCDs—is referred to as nutritional care. Nutritional care is defined
as nutritional assessment, diagnosis, intervention, monitoring, and
evaluation, according to the Nutrition Care Process Model, which is
supported by the Academy of Nutrition and Dietetics. Using carefully
gathered, comprehensive, and pertinent data regarding a patient’s
diet, nutritional assessment determines the issue. The next step is to
administer the proper nutritional therapy if malnutrition is found or
diagnosed. “A supportive process, characterized by a collaborative
counsellor-client relationship, to establish food, nutrition, and
physical activity priorities, goals, and action plans that acknowledge
and foster responsibility for self-care to treat” is how nutritional
counselling is described as one facet of nutritional intervention
characterized by a collaborative counsellor-client relationship, to
establish food, nutrition, and physical activity priorities, goals, and
action plans that acknowledge and foster responsibility for self-care
to treat an existing condition and promote health.”[12]
Because they frequently interact with patients and are familiar
with their social environments and medical histories, primary care
physicians (PCPs) and health consultants are a popular source of
health information. Because they think health consultants are the
most qualified, trustworthy, and personable sources of nutritional
information, patients look forward to receiving nutritional advice
from them.Consequently, general practitioners have the opportunity
to positively influence the behavior and lifestyle choices of their
patients.[7,13,14]Thus, this study aims to provide an overview of
the current state of knowledge, attitudes, and practices related to
nutritional care and nutritional counselling in health, as well as
barriers to nutritional counselling.
Methodology
Methodology:A structured survey was conducted to assess the
practices, attitudes, and understanding of nutrition counselling
among health consultants from a range of medical specialities,
including Intensivists, Nephrologists, Neurosurgeons, Diabetologists,
Dietitians, Gastroenterologists, and OncologistsTo collect both
quantitative and qualitative data, the survey comprised both multiple choice
and open-ended questions. The questions were created to
address a variety of nutrition-related subjects, such as attitudes
towards public nutrition, knowledge of important nutrition concepts
(such as dietary guidelines, malnutrition, and diseases linked to
nutrition), and confidence in giving nutritional advice.
Data was collected and analyzed to identify trends and correlations
between knowledge and attitudes, as well as to assess any gaps in
nutrition education and the barriers to providing effective nutrition
counseling. Theresponses were analyzed using both qualitative and
quantitative methods to provide a comprehensive overview of how
nutrition counseling is currently practiced among health consultants
and to identify areas where additional support and education are
needed.
Result and Discussions
Nutritional knowledge refers to the ability to understand essential
information about diet, nutrients, and their influence on overall
health and well-being.[15] It plays a crucial role in healthcare, as
physicians with a strong foundation in nutrition are better equipped to
identify dietary risk factors, provide effective nutritional counseling,
and implement preventive strategies to reduce the incidence of
nutrition-related diseases. Proper nutritional knowledge also allows
healthcare professionals to guide patients in managing conditions
such as obesity, diabetes, cardiovascular diseases, and malnutrition,
ultimately improving patient outcomes.[16]
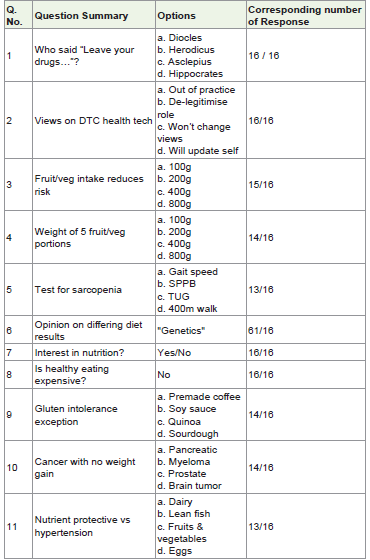
In this study, a structured questionnaire consisting of 28 items
was developed (depicted in[Table 1] to assess the level of nutritional
knowledge among 16 medical consultants. Prior to distribution, the
consultants were informed about the study’s objectives and provided
their consent to participate.
The questionnaire aimed to evaluate their understanding of
dietary recommendations, nutrient functions, and the role of
nutrition in disease prevention and management.The responses reflect
a consistently high level of interest and a positive outlook toward
nutrition among the participants, highlighting their recognition of its
critical role in improving patient outcomes. A majority affirmed the
inclusion of nutrition assessment and counselling as part of standard
clinical practice and expressed confidence in their ability to provide
basic nutrition advice.The significant questions and answers are
summarized below.
A) Nutrition Knowledge
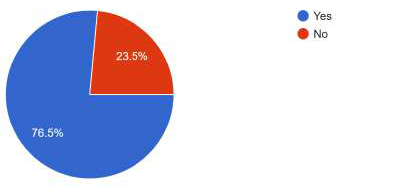
• Question: Who advised the physicians in 400 BC: “Leave
your drugs in the chemist’s pot if you can heal your patient with
food”?
Analysis: Most respondents (76.5%)(Graph 1) accurately credited
Hippocrates with this viewpoint, demonstrating a keen understanding
of his impact on early medical theory. There may be a knowledge
gap, nevertheless, as the remaining percentage of participants were
unfamiliar with this historical background. This implies that including
historical perspectives on nutrition into medical education could
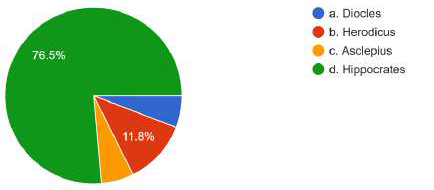
improve doctors’ comprehension of the established link between diet
and health, highlighting the significance of nutrition in contemporary
clinical practice.
• Question: How much daily intake of vegetables/fruits is
associated with a reduced risk of cardiovascular diseases?
Analysis:47.1% of participants in this survey chose 400g
correctly,(Graph 2)indicating a modest level of knowledge about
evidence-based dietary recommendations. Although this suggests
that most participants are aware of global health guidelines, 53% of
them either overestimated or underestimated the necessary intake,
suggesting a possible knowledge gap. Enhancing nutritional education
could raise awareness and promote adherence to the recommended
intake of fruits and vegetables for cardiovascular health benefits.
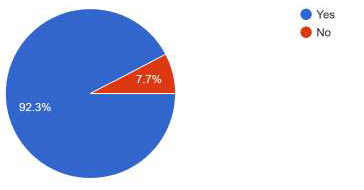
• Question: Does early nutrition intervention reduce
treatment recovery time and hospital stays?
Analysis:There is broad agreement regarding the significance of
early nutrition care in patient recovery, as seen by the majority (92.3%)
of respondents’ “Yes” responses. (Graph 3) This shows that the clinical
advantages of prompt nutritional intervention are understood. But
it’s crucial to make sure that this knowledge is applied to regular
clinical practice. Additional patient outcomes and cost savings can be
achieved by ongoing education and hospital policies that place a high
priority on nutrition assessment and intervention.
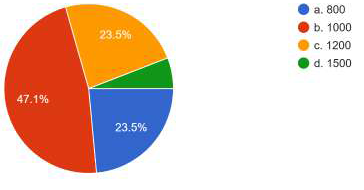
• Question: What is the recommended calcium intake for
women aged 51–70 years?
Analysis:47.1% of respondents correctly selected 1,000 mg, which
is lower than the recommended amount.(Graph 4)This suggests
a need for clearer communication and reinforcement of official
calcium recommendations, particularly for postmenopausal women,
who require higher calcium intake to mitigate the risk of osteoporosis
and fractures. Providing targeted educational resources can help
improve adherence to evidence-based dietary guidelines in both
clinical practice and public health messaging
Portion Size Equivalence:
• Question: What weight is equivalent to five portions of
fruits/vegetables?
• Analysis:The majority of respondents (64.7%)(Graph 5)
correctly selected 400 grams, reflecting a reasonable level of awareness
regarding portion recommendations. However, some responses
indicated 100 grams or 200 grams, suggesting misconceptions about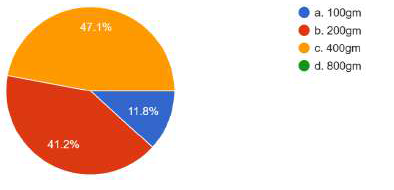
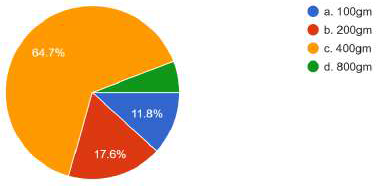
portion sizes or daily intake recommendations. This variability
highlights the need for clearer nutrition education on portion sizes
and the importance of consuming a diverse range of fruits and
vegetables to meet dietary guidelines. Standardizing portion size
education can help individuals make more informed dietary choices
and improve adherence to health recommendations
Sarcopenia Evaluation:
• Question: Most convenient test to predict sarcopenia related
outcomes?Analysis:Responses were divided between SPPB, TUG and
Gait speed reflecting a familiarity with both assessment tools
among respondents. However, majority of the respondent (35.3%)
(Graph 6) selected SPPB, which is often considered more clinically
comprehensive for predicting sarcopenia-related outcomes.
The presence of mixed responses highlights the need for further
clarification on the most appropriate tests for different clinical
scenarios. Educating healthcare professionals on the strengths and
applications of various sarcopenia assessment tools can enhance early
detection and management strategies.
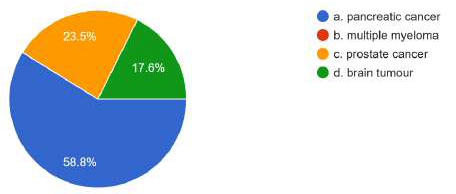
Cancer and Weight Gain:
• Question: Which type of cancer is linked with no weight
gain in patients?
Analysis:The majority of responses (58.8%) (Graph 7)identified
pancreatic cancer, aligning with its well-documented link to cachexia
and weight loss. However, the mention of prostate cancer suggests
some variability in understanding the weight-related effects of
different cancers. This indicates a potential need for further education
on the metabolic impact of various cancers to ensure accurate clinical
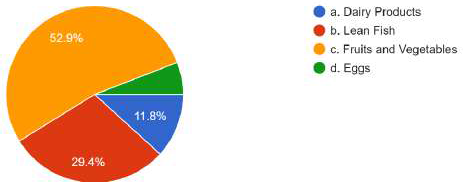
assessments and patient counseling.Nutrients Protective Against Hypertension:
• Question: Which nutrient helps in hypertension
prevention?
Analysis: Most common answer by majority participants (52.9%)
(Graph 8) was Fruits and Vegetables. Some answers mention Lean
Fish or Dairy Products. Fruits and vegetables are rich in potassium,
which is beneficial for hypertension management, making this the
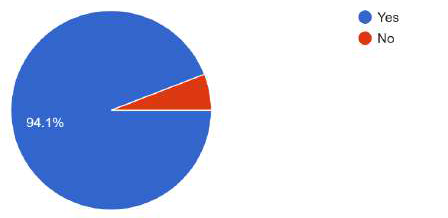
correct response.Malnutrition:
• Question: Is severe acute malnutrition a medical
emergency?
Analysis:The Majority response (94.1 %) of “Yes”(Graph
9)highlights a strong understanding of the critical nature of
malnutrition in healthcare. Recognizing SAM as a medical emergency
ensures timely intervention, appropriate refeeding strategies, and
supportive care, ultimately improving patient survival and recovery
outcomes. Continued education and awareness on early detection,
proper management, and long-term nutritional support can further
strengthen healthcare responses to SAM.
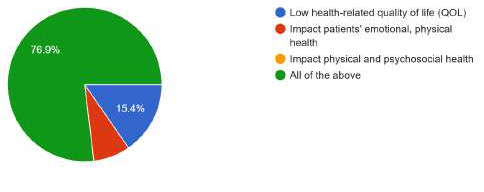
• Question: How does malnutrition impact morbidity,
hospital stays, and functional capacity?
Analysis:The majority of respondents (76.9%) (Graph 10)
correctly identified all of the above as impacts of malnutrition,
demonstrating a strong awareness of its comprehensive effects
on health outcomes. This aligns with established clinical evidence
showing that malnutrition is a major contributor to increased
morbidity, longer hospital stays, and reduced functional capacity.
Continued education on nutritional screening, early intervention,
and personalized care plans can help mitigate these adverse effects
and improve patient outcomes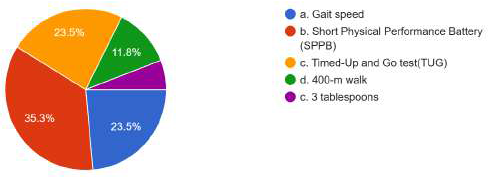
B) Attitudes and Practices
• Question: Are respondents confident in providing
nutrition advice?
• Analysis:Of the respondents, 76.5%(Graph 11) think they
are competent enough to advise patients on diet. This suggests that the
majority of responders are assured of their knowledge and ability to
counsel patients on issues concerning diet. This implies that some of
the respondents could need more instruction, training, or assistance
in order to feel confident in their dietary advice.
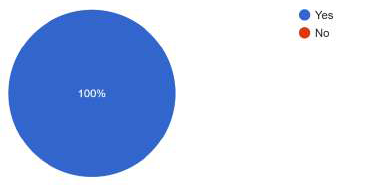
• Question: Patient motivation is the most essential
component to achieving dietary change and needs a psychologically
powered intervention
• Analysis:As seen in Graph 12, all the respondents
emphasized the importance of patient motivation, reflecting a
strong recognition of the role psychological factors play in dietary
counseling. This view underscores the need for patient-centered
approaches that go beyond simply providing nutritional information
and instead focus on fostering the patient’s intrinsic motivation to
make meaningful changes. Such approaches, tailored to the patient’s
unique situation, are more likely to lead to sustained dietary change
and improved health outcomes. This aligns with best practices in
behavioral nutrition and emphasizes the importance of integrating
psychological and emotional support into clinical nutrition care.
• Question: Do you have special interest in nutrition for
your kind of practice? If yes, how much time does the patient get
for nutrition counselling? In how many sessions, the first/ only a
few/ all visits to your clinic? If no, why not? lack of time / lack of
confidence / lack of resources with adequate nutrition knowledge
• Analysis:Practices regarding nutrition counseling vary
significantly across consultants, with many citing time constraints
as the primary barrier to effective nutrition intervention. This
underscores the need for more structured time allocation in
clinical practice to facilitate comprehensive nutrition counseling.
Additionally, there may be a gap in nutrition education for healthcare
providers, which could hinder their confidence in delivering detailed
dietary advice. Addressing these challenges could involve integrating
nutrition training into medical education and enhancing resource
availability for practitioners, ensuring that nutrition counseling is an
integral part of patient care
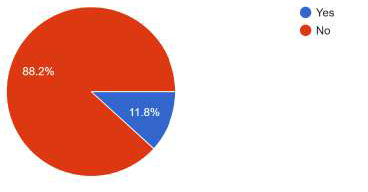
• Question: Is healthy eating expensive and only for the
wealthy?
• Analysis:The responses as depicted in (Graph 13), reflect
an optimistic outlook, indicating a belief that healthy eating can be
accessible to all, regardless of socioeconomic status. However, in
practice, the affordability of healthy eating can vary significantly
based on factors such as location, access to food stores, and personal
financial resources. Addressing these disparities may require
community-based initiatives that promote access to healthy food
and support education on budget-friendly nutrition. Ensuring that
healthy eating is accessible to all is critical to improving public health
outcomes.
The survey’s findings provide insightful information about the
state of nutrition counselling in medical settings today. The findings
reveals a notable lack of standardization and trust on some practical
aspects of nutrition therapy, such as clinical nutrition tools and serving
sizes, even though the majority of health consultants acknowledge the
significance of evidence-based dietary advice. This variation implies
that although most consultants understand the value of nutrition,
they apply this understanding inconsistently, which could affect the
standard and efficacy of patient care. All patients could receive highquality,
evidence-based nutritional guidance if nutrition counselling
procedures are streamlined throughout the healthcare system with
the support of standardized training that fills in these gaps.[17]
The survey’s findings also show a definite proactive attitude to
treating malnutrition and teaching patients about healthy eating,
despite the difficulties. Everyone agrees that nutrition is important
for patient health, especially when it comes to treating or avoiding
malnutrition, which is strongly associated with negative health
outcomes.[18]Although consultants show a great commitment to
inspiring patients, there were noticeable inconsistencies in their
counselling techniques and confidence gaps. A need for more
thorough and specialized training is evident from the fact that many
health experts are uncertain of how to consistently provide dietary
counselling. [19]
One of the study’s main conclusions is that there are wide
variations in the knowledge, attitudes, and practices of health
consultants with relation to nutrition counselling. Attention is
needed in the areas of resource allocation and self-esteem. Due to a
lack of resources or training, many consultants may feel unprepared
or unconfident when offering comprehensive nutritional advice.[20]
This emphasises the necessity of funding professional development
in order to increase consultants’ sense of self-worth and make sure
they feel prepared to manage the dietary components of patient
care. Furthermore, increasing funding for things like support
systems and nutritional tools could enhance the standard of care
and boost the trust that medical professionals have in their dietary
recommendations.[21]
Nutrition counselling needs to be encouraging, interesting, and
tailored to each patient in order to be more successful. Health experts
should have an open mind while discussing nutrition and adjust their
recommendations based on each patient’s unique needs. Because
dietary requirements differ greatly from person to person and a onesize-
fits-all strategy is frequently ineffective, this personalization is
especially crucial. In particular, primary care doctors are crucial to the
early prevention of diseases linked to food. Primary care physicians
can serve as the first line of defence against conditions like diabetes,
hypertension, and obesity, which are frequently preventable with
dietary and lifestyle modifications, by offering fundamental nutrition
advice and promoting healthy eating habits. It is equally crucial,
though, that doctors understand the boundaries of their knowledge
in nutrition and can, when needed, refer patients to dietitians or
nutritionists. This guarantees that patients receive the most precise,
focused dietary guidance in accordance with their unique medical
requirements.[22]
Additionally, doctors need to be aware of how important diet
is for both preventing and treating illness. Healthcare providers
will be better able to offer their patients comprehensive care if they
acknowledge the critical role that diet plays in controlling chronic
illnesses. This entails treating the double burden of malnutrition,
resolving patient food insecurity, and preventing noncommunicable
diseases that result from unhealthy eating patterns.[23]Medical
professionals need to be educated to identify the symptoms of lifestyle
diseases and malnutrition and to include nutritional counselling in
their treatment regimens.[24]
Personalized therapies are a key component in enhancing
clinical nutrition results. Instead of following a general set of dietary
recommendations, medical professionals need to be prepared to
evaluate the particular needs of every patient. When establishing
dietary recommendations, it is important to take into account
several factors, including age, gender, socioeconomic situation,
cultural preferences, and medical history. In addition to encouraging
increased patient involvement, this tailored approach increases
the probability that patients would follow the suggested dietary
modifications, improving health outcomes.[22]
For example, individuals with long-term conditions like
diabetes might need more detailed dietary advice on controlling
blood sugar, whereas those who are malnourished or losing weight
might require more thorough nutritional rehabilitation. Patients
who receive personalized nutrition counselling are more equipped
to make decisions that support their own health objectives and
have an understanding of how dietary modifications can be used to
manage their unique medical problems. Healthcare practitioners may
guarantee that patients receive individualized care that meets both
short-term and long-term health needs by working with dietitians
and other nutrition specialists.[20]
Conclusion
The results of this survey highlight the need for a more
standardized and certain method of nutrition counselling in
medical settings. To give good dietary recommendations, healthcare
professionals—especially primary care physicians—need to have the
requisite education, tools, and self-assurance. Specialized nutrition
education is a clear chance for professional growth, enhancing
knowledge, fostering self-worth, and guaranteeing consistency in
counselling techniques.[21]
Personalized and proactive nutrition counselling must be
integrated into clinical practice for the broader healthcare system to
effectively address the rising prevalence of diet-related illnesses and
malnutrition. In order to play a significant role in preventing chronic
diseases and encouraging their patients to lead healthier lifestyles,
doctors and health advisors must also understand the significance
of nutrition in disease prevention. Health consultants can improve
public health outcomes and eventually save healthcare costs by
delaying the emergence of lifestyle-related disorders through the
integration of nutrition into patient care.[23]
Investing in improved nutrition education, more funding, and
interdisciplinary cooperation will give medical practitioners the
groundwork they need to improve clinical nutrition results and
patients’ general health.[24]
Acknowledgments:
Authors, thank all the participants (Dr.
Kaustubh V Shendkar, Dr. Sachin Patil, Dr. Bhushan Nagarkar,
Dr. Prashant Sakhavalkar, Dr. Nana Kunjir, Dr. Muddassir Sheikh,
Dr. Jitendra Khandge, Dr. Aditya Gudhate, Dr. Sharad Biradar,
Dr. EppaVimalakar Reddy, Dr. Gopi Krishna, Dr. Sujatha Stephen
Konda, Dr. Shravani Thakur, Dr. Ravinder Samudrala, Dr. Swaroop
Verma, Dr. Ramesh Hasani, Dr. Diwakar Pandey, Dr. Vinod Gosavi,
Dr. Amol Kulkarni, Dr. Vinit Birajdar, Dr. Akshay Shivchhand, Dr.
Ajit Kumar Singh, Dr. Akash Roy, Dr. Sayan Paul, Dr. Banigallapati
Vijay Kiran,Dr. Satish Sarode)for their enormous support in the
study.Conflict of interest:Author(s) declare(s) that there is no conflict
of interest
References
Citation
Basu D, Ghosh S, Kumar S, Sinhababu S, Singh N. Knowledge, Attitudes, and Practices in Nutrition Counselling: A Survey Analysis among Health Consultants. Indian J Nutri. 2025;12(2): 315.